A Rare Case of Recurrent Paget’s Disease of the Vulva and Gluteal Region Treated with Radiation Therapy
Images









CASE SUMMARY
An 80-year-old woman presented to us in May 2018 with a large cutaneous growth involving the vulva and gluteal region (Figure 1). A detailed clinical history revealed that in 2012, she initially noticed a nonhealing growth over the vulva and gluteal region for which she underwent wide local excision with skin grafting. The histopathology report was suggestive of Paget’s disease, and her surgeon advised close follow-up. In 2015, local recurrence was detected and she underwent a second surgery. Histopathology showed features of extramammary Paget’s disease (EMPD) with focal stromal invasion. The patient was again advised for close follow-up.
In May 2018, local recurrence was again detected. Biopsy showed poorly differentiated carcinoma with pagetoid spread to the epithelium. Immuno-histochemistry (IHC) showed features consistent with Paget’s disease with extensive pseudoepitheliomatous hyperplasia. The patient’s primary surgeon deferred any further surgical intervention and recommended radiation therapy. A positron emission tomography – computed tomography (PET-CT) scan was performed to detect nodal involvement and to rule out synchronous malignancy. The PET-CT scan showed iliac and inguinal nodal metastasis but did not show evidence of synchronous malignancy.
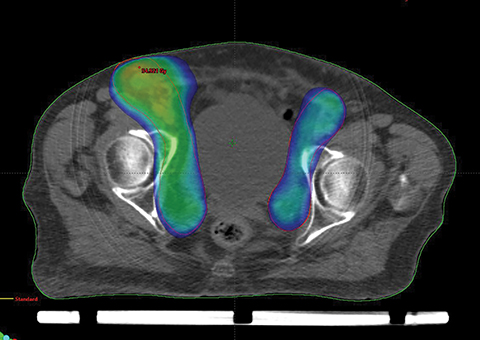
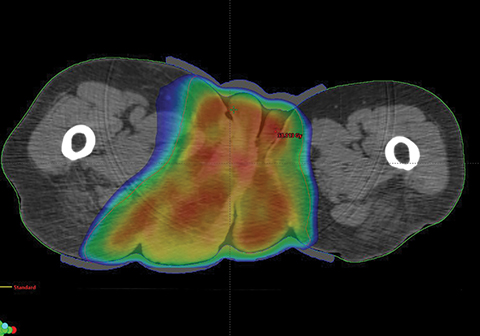
The patient was treated with volumetric-modulated arc therapy (VMAT) (RapidArc; Varian, Palo Alto, California) using 6-MV photons in a sequential manner to a total dose of 56 Gy in 28 fractions, 2 Gy per fraction, delivered 5 days per week (Figure 2).
Treatment plan details include:
- The clinical target volume (CTV) primary = the gross tumor volume (GTV) primary (based on clinical examination and PET-CT) + a 2-cm margin. The CTV node = the bilateral common + external + internal iliac + bilateral inguinal nodal region.
- PTV = CTV + 5 mm.
- Phase 1: PTV primary + Node: 42 Gy in 21 fractions, 2 Gy per fraction.
- Phase 2: PTV primary + gross nodal volume [(GTV) node + 5 mm]: 12 Gy in 6 fractions, 2 Gy per fraction.>
- Phase 3: Planning target volume (PTV) primary: 2 Gy in 1 fraction, 2 Gy per fraction.
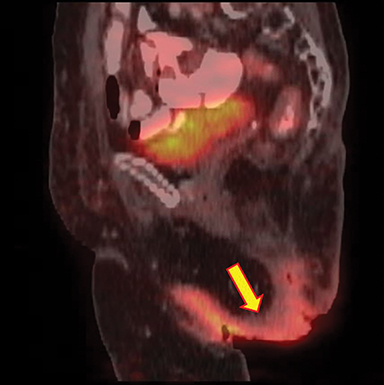
A 5-mm gel bolus was placed over the primary tumor site for dose build-up over the cutaneous surface. The patient also received concurrent oral capecitabine 500 mg twice daily as a radiation sensitizer. Considering her age and frail general condition, the medical oncologist preferred oral capecitabine (in low dose as a radiation sensitizer) over other more toxic chemotherapy options. The patient tolerated the treatment well with grade 3 acute skin and mucosal reactions over the ano-genital region. These acute effects recovered well within 4 weeks of completing treatment. Disease response assessment performed at a 2-month and 5-month follow-up visit showed good local control and the patient symptomatically felt much better. Figure 3 shows clinical response during and after treatment. PET-CT performed at a 1-year follow-up showed no evidence of residual locoregional disease (Figure 4).
IMAGING FINDINGS
Pre-radiation therapy whole-body PET-CT (Figure 4) showed a large metabolically active growth involving the skin of right gluteal region, extending anteriorly up to the inguinal region, perianal region and vulva with a standard uptake value (SUV) max of 7.73. Mildly F-18 fluorodeoxyglucose (FDG)-avid enlarged bilateral common iliac, bilateral external iliac and right inguinal lymph nodes, the largest measuring 3.8 × 1.6 cm with an SUV Max of 3.34, suggestive of nodal involvement. There was no distant metastasis. Post-treatment PET-CT (at 1-year follow-up) showed complete locoregional radiological and metabolic response.
DIAGNOSIS
EMPD of the vulva and gluteal region
The differential diagnosis in the ano-genital area includes neurodermatitis, psoriasis, seborrheic dermatitis, lichen simplex, lichen planus, mycosis fungoides, Bowen’s disease and periorificial tuberculosis.1 Histopathologically, the differential diagnosis includes pagetoid Bowen’s disease and pagetoid malignant melanoma in situ.2
DISCUSSION
EMPD is a rare dermatologic condition that frequently presents in areas where apocrine sweat glands are abundant such as the vulva, perineum, scrotum and penile skin. EMPD has a female predominance and usually occurs in the sixth to eighth decade of life.3
The common presenting symptoms include pruritus, bleeding, oozing, tenderness, a painful burning sensation or hypopigmented lesions.4 Lesions clinically present as erythematous, well-demarcated plaques that may become erosive, ulcerated, scaly or eczematous.5 There are usually 3 patterns of EMPD: (1) an in situ epithelial form without associated carcinoma; (2) an epithelial form with associated adnexal carcinoma; and (3) a form associated with visceral malignancy of the genitourinary or gastrointestinal tract.1 There is a strong association between the presenting anatomical site of EMPD and the underlying visceral carcinoma.6
Due to the histologic extension beyond the clinically abnormal area, local recurrence of EMPD is relatively common. EMPD cells have the potential to invade the dermis and to metastasize. Hard nodules and regional lymph node enlargement may develop, resulting from underlying carcinoma. “Underpants-pattern erythema” is a specific clinical aspect of genital EMPD.3
Surgery is the gold standard treatment for patients with EMPD. Other therapies include radiation therapy, curettage, topical fluorouracil (5-FU), and cryosurgery.5 Systemic chemotherapy (vincristine, docetaxel, carboplatin, 5-FU, mitomycin-C, etoposide) can be used if there are contraindications to surgery and radiation therapy.3 Radiation treatment can be utilized for inoperable lesions. A systematic review of the role of radiation therapy in EMPD evaluated 19 articles published from 1991 to 2015.7 Radiation therapy was used in different clinical settings, namely the definitive, postoperative adjuvant, salvage and preoperative settings. The doses were 30 to 80 Gy in 3 to 43 fractions for gross disease, 32 to 64.8 Gy in 20 to 30 fractions for adjuvant treatment, and 40 Gy in 20 fractions for preoperative treatment. For definitive and salvage radiation therapy, response rates were 50% to 100% with 0% to 80% relapse rates. The dose-response relationship suggested a dose of at least 60 Gy for treating gross disease. A report on long-term outcomes of EMPD treated with definitive radiation therapy with doses of 40 to 56 Gy in 10 to 28 fractions showed an initial complete remission rate of 85%. The local relapse rate was 28.6% at a median follow-up of 6 years.8
A study by Hata et al reported the outcomes of radiation therapy for 41 patients of genital EMPD.9 Radiation therapy doses of 45 to 80.2 Gy (median 60 Gy) in 23 to 43 fractions were utilized. Local progression-free survival and disease-free survival were 88% and 55% at 3 years and 82% and 46% at 5 years, respectively. Tumor invasion into the dermis and nodal metastasis were significant prognostic factors for distant metastasis and survival.
A literature review from the Cochrane Register of Controlled Trials, MEDLINE and the EMBASE database up to September 2015 concluded that radiation therapy alone is an alternative therapeutic approach for extensive inoperable disease.10 High-risk features warranting adjuvant radiation therapy (after primary surgery) include dermal invasion, lymph node metastasis, close or positive surgical margins, large tumor diameter, multifocal lesions, coexisting histology of adenocarcinoma or vulvar carcinoma, high Ki-67 expression, adnexal involvement, and overexpression of HER-2/neu. A case report of suprapubic EMPD treated with electron-beam radiation therapy to a dose of 60 Gy in 30 fractions showed excellent local response.11 Debabrata et al reported a case of EMPD of the vulva treated with surgery followed by adjuvant radiation therapy with good local control at 20 months’ follow-up.12 Seok-Hyun et al reported their experience in treating 3 cases of EMPD of the vulva with definitive radiation therapy (54 to 78 Gy in 1.8 Gy per fraction) and found complete response in all cases.13 A case report on EMPD of the vulva treated with surgery followed by adjuvant radiation therapy (50.4 Gy in 28 fractions) with concurrent weekly cisplatin (40 mg/m2) showed good local control at 15-months’ follow-up.14 Leslie et al from the Mayo Clinic Cancer Center reviewed cases of metastatic EMPD treated from 1998-2012 and supported use of local radiation therapy for bulky disease sequentially with chemotherapy (carboplatin and paclitaxel or irinotecan).15
This case report adds to the existing slim body of literature on the role of definitive radiation therapy in EMPD of the vulva. It demonstrates how effective and safe radiation therapy can be in controlling even grossly bulky disease. Concurrent capecitabine as a radiation sensitizer can be considered in elderly frail patients not considered suitable for other more toxic chemotherapy regimens. Treatment planning with VMAT helps to deliver a conformal dose distribution to the irregular target geometry, which includes the primary cutaneous site and nodal region Hence, radiation therapy can be considered as an effective and safe alternative to surgery in such cases.
CONCLUSION
EMPD is a rare cutaneous disease of elderly patients. Clinical and radiological evaluation is of paramount importance to detect underlying visceral malignancy. Surgery is the preferred primary treatment; however, local recurrences are common. Repeat surgery (which is often extensive) in the elderly population subset is difficult and carries significant morbidity. Radiation therapy is a safe and effective nonsurgical treatment modality for these patients. Even for bulky disease, radiation therapy can result in gratifying local control as demonstrated in this case report.
REFERENCES
- Helwig EB, Graham GH. Anogenital (extramammary) Paget’s disease. a clinicopathologic study. Cancer. 1963;16:387-403.
- Kirkham N. Tumours and cysts of the epidermis. In: Elder D, Elenitsas R, Jaworksy C, Johnson B Jr, eds. Lever’s Histopathology of the Skin. 8th ed. Lippincott- Raven; 1997:736-738.
- McDaniel B, Brown F, Crane JS. Extramammary Paget disease. [Updated 2019 December 17, 2019]. In: StatPearls [Internet]. StatPearls Publishing; 2019. https://www.ncbi.nlm.nih.gov/books/NBK493224/. Accessed on December 19, 2019.
- Balducci L, Crawford ED, Smith GF, Lambuth B, McGehee R, Hardy C. Extramammary Paget’s disease: an annotated review. Cancer Invest. 1988;6:293-303.
- Banerjee S, Chatterjee M, Chand K. Extramammary Paget’s disease. Indian J Dermatol Venereol Leprol. 2005;71:417-420.
- Chanda JJ. Extramammary Paget’s disease: Prognosis and relationship to internal malignancy. J Am Acad Dermatol. 1985;13:1009-1014.
- Tagliaferri L, Casa C, Macchia G, et al. The role of radiotherapy in extramammary Paget disease: a systematic review. Int J Gynecol Cancer. 2018;28(4):829-839.
- Tackenberg S, Gehrig A, Dummer R, Navarini AA. External beam radiotherapy of extramammary Paget disease. Cutis. 2015;95:109-112.
- Hata M, Koike I, Minagawa Y, et al. Radiation therapy for extramammary Paget’s disease: treatment outcomes and prognostic factors. Ann Oncol. 2014;25(1):291-297.
- Tolia M, Tsoukalas N, Sofoudis C, et al. Primary extramammary invasive Paget’s vulvar disease: What is the standard, what are the challenges and what is the future of radiotherapy? BMC Cancer. 2016;16:563.
- Valle L, Deig C, Wright R, High W. An advanced case of extramammary Paget disease: safe and effective treatment in an inoperable elderly patient using extensive en face electron irradiation. JAAD Case Rep. 2019;5:72-74.
- Barmon D, Kataki AC, Imchen L, Sharma JD. Extramammary Paget’s disease of vulva. J Mid-life Health. 2012;3:100-102.
- Son S, Lee J, Kim Y, et al. The role of radiation therapy for extramammary Paget’s disease of the vulva; experience of three cases. Cancer Res Treat. 2005;37(6):365-369.
- Inayama Y, Abiko K, Miyamoto T, et al. Invasive Paget’s disease of the vulva treated with a combination of surgery and concurrent chemoradiotherapy: a case report. Molec Clin Oncol. 2018;9:489.
Citation
MA A, M B, P M, S S, KR M, S P, PA S, SP V, AKR G, D K. A Rare Case of Recurrent Paget’s Disease of the Vulva and Gluteal Region Treated with Radiation Therapy. Appl Radiat Oncol. 2020;(1):44-47.
April 4, 2020