A review of strategies for optimizing workflow, quality improvement, and patient safety within radiation oncology departments
Images

SA-CME credits are available for this article here.
Safety challenges within the field of radiation oncology have gained increasing attention in the mainstream media and among organizations such as the Food and Drug Administration (FDA), American Society for Radiation Oncology (ASTRO), and the American Association of Physicists in Medicine (AAPM) over the last decade.1,2 Prior data has suggested that changes in workflow, transfer of misinformation, increasing workload of radiation oncology services and complexity of treatment delivery are frequent sources of errors, underscoring the importance of established processes for patient safety and mechanisms for quality improvement for ensuring the safe delivery of radiation therapy.3-6
Patterns of care recommendations are outlined in the American College of Radiology (ACR) Appropriateness Criteria and the National Comprehensive Cancer Network (NCCN) guidelines; however, dedicated procedures at the departmental and institutional level are essential as well.2 The ACR Practice Parameters discuss typical components of a quality improvement program including peer review, periodic auditing of radiation oncology medical records, review of physics quality improvement, review of incident reports and deviations, and patient outcomes.2 Suggested components include new patient review, chart review (both clinical and physics), image verification review, and incident reporting and learning system to facilitate quality improvement projects. The International Atomic Energy Agency (IAEA) has identified that optimization of patient safety within radiation therapy require personnel-, system-, and equipment-level initiatives.4 Voluntary error reporting systems and comprehensive quality assurance programs have been shown to significantly decrease error rates within radiation oncology.7 This article will review areas susceptible to error within radiation oncology workflow, present primarily personnel- and system-level initiatives implemented within our department and other institutions to mitigate errors and enhance safety, and to describe efforts to incorporate quality improvement and patient safety into resident education.
Incident Reporting Systems
The systematic documentation, reporting and analysis of incidents is a critical first step in the quality improvement process. A national system for incident reporting within radiation oncology has been proposed by the Canadian Partnership for Quality in Radiation (CPQR) therapy to standardize taxonomy and classification of severity of incidents. A list of 26 core elements was generated, which included event description, severity classification with a medical acute injury and dosimetric scale, hazards, and mitigating factors, and was reviewed by a panel of experts for consensus.8 Similarly, ASTRO and AAPM implemented the Radiation Oncology Incident Learning System (RO-ILS) in 2014, with 425 facilities across the United States, which facilitates collection of incidents within a national database with generation of quarterly aggregate reports on events throughout the country with suggestions on process improvement.6,9 As there is likely variation across institutions regarding descriptions and classifications of incidents, initiatives such as these serve as a model for a systematic method for incident reporting, which can improve multi-institutional data collection and implementation of interventions across systems.
The Workflow Enhancement (WE) Team serves, in part, as a structured reporting system for incidents and errors specific to our department, separate from our institution’s incident reporting system.10 Errors are reported anonymously online through the department’s intranet site or can be reported at the biweekly process improvement meeting. Errors can be reported by physicians, radiation therapists, dosimetrists, medical physicists, residents, nurses, and administrative staff. Forms contain patient identifiers, including name and medical record number, error category/type, and description of the error, and all forms are recorded into a secure Excel database. An analysis of all incidents submitted to the WE Team in 2013 demonstrated 10 incidents. The number of patients treated per day was significantly associated with increased risk of incidents (p < 0.003) and the ratio of patients to physicians was significantly associated with errors (p < 0.03).5 Increased workload as a risk factor for error has been identified within other institutional reporting systems as well.11 Additionally, communication breakdown and changes in workflow are also well-established sources of error in the literature.3-6 Workflow processes, communication protocols, systematic checks to mitigate these sources of errors and departmental stressors are discussed below.
Implemented Initiatives
CT Simulation Time-out/Checklist Procedure
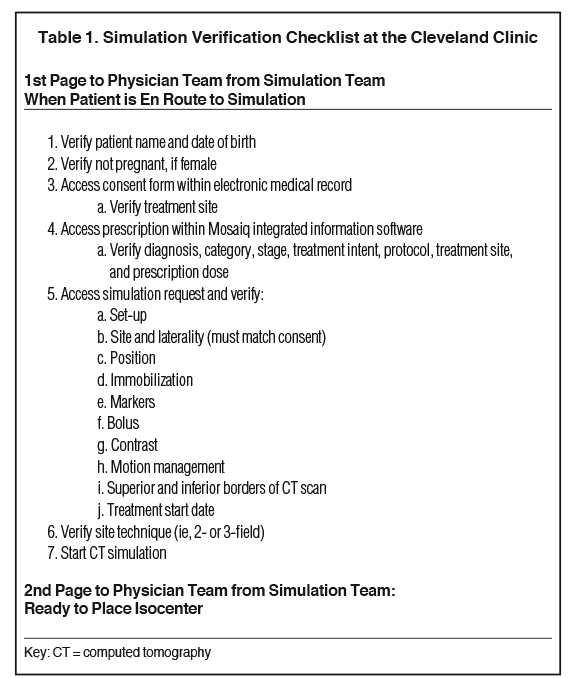
The efficacy of safety checklist procedures in reducing errors is well established in the surgical literature and is now a national patient safety goal standard.7,12 The computed tomography (CT) simulation procedure is one of the first steps within the radiation therapy treatment planning process and its accurate completion is critical. Failure to complete this step can lead to substantial downstream effects, including additional, unnecessary testing; patient treatment delays; and errors in treatment delivery. An analysis of incident reports through the WE Team at our institution identified 136 simulation-related events reported between 2014 and 2016. Examples of simulation-related events included wrong site imaged, failure to administer contrast, failure to place mouthpiece, etc. A safety checklist and time-out procedure were implemented to address the errors noted in the simulation process. A pocket safety checklist card was distributed to all physicians (Table 1) and verbal communication between the radiation therapist and physician was required prior to the patient’s simulation.13 One year after implementation of this safety procedure, the number of simulation-related events reported to the WE Team decreased by 57% (p < 0.0001).13 Specific safety checklists have now been introduced for prostate and gynecologic brachytherapy, intraoperative radiation therapy (IORT), and stereotactic radiosurgery (SRS) procedures.
Quantitative Metric and Automatic Auditing Program (QMAP)
Process consistency, automation, workflow standardization, and frequent checks and reminders are effective mechanisms for reducing errors and streamlining processes involving multiple teams. At our institution, our incident reporting system identified timely checks of cone-beam CTs, plan completion, weekly physics checks, and weekly physician on treatment visits, as areas of improvement, with quarterly late checks of these tasks ranging from about 6% to 15%. Timely and accurate completion of these tasks is imperative to identifying potential errors and optimizing patient safety. To mitigate this, our department implemented a Quantitative Metric and Automatic Auditing Program (QMAP). Acceptable time frames for completing each task were agreed upon. A software program was developed using Mosaiq (Elekta, Stockholm, Sweden) integrated information software to generate an automatic timestamp upon completion of each critical clinical task, as well as reminders if a task was not completed. In addition to reminding the responsible party, a designated triage team is also notified to help mitigate a workflow delay before it occurs. The rates of timely completion of daily and weekly metrics before and after QMAP implementation are summarized in Table 2.
Similarly, the University of Michigan reported on the development of a Plan-Checker Tool (PCT) within the Eclipse Scripting Application Programming Interface (Varian, Palo Alto, California) as another effort to automate workflow, improve efficiency, and reduce treatment delays.14 Their software includes a system of automated and manual checks of a plan’s suitability for treatment. The highest frequency error identified was within the category of secondary check software, with examples including a plan not exported to the treatment planning system and a reference point not having a location to calculate MUs (18%). Other examples include a mislabeled field name, scheduling errors, and plan and prescription inconsistencies. They were able to automate 19 of 33 checklist items, which led to a 60% reduction in the number of patient delays due to errors in the treatment planning process after 6 months of PCT implementation. PCT did not reduce the number of errors found during the physics check; however, it increased the identification of errors that help avoid treatment delays and, most importantly, potential errors in treatment delivery.14 Automation is an important tool for improving quality and workflow.
Structured Peer Review
Across providers, there can be substantial variability in patient positioning, target volume delineation, choice of dose fractionation, and normal tissue dose constraints within the radiation treatment planning process. The AAPM and the European Organization for Research and Treatment of Cancer (EORTC) have recommended quality assurance rounds with treatment plan peer review to ensure patient outcomes are not affected by interprovider variability.15 The impact of structured peer review is well illustrated by a study of 1,247 plans reviewed in quality assurance rounds from 2004 to 2010 in a Canadian radiation oncology department. Plans were peer reviewed and graded as being adequate (A), needing minor suggestions of change to a plan for a future patient (B), or requiring significant change before delivery of the next fraction (C). They determined that 6% of plans were graded B and 1% were grade C and that mean years of experience were less for the plans graded C compared to those graded A (p = 0.02), highlighting the importance of peer review for physician education.16 Treatment plan peer review often occurs after a patient has started treatment, so as to avoid treatment delays. Despite increased logistical concerns, there may be value in prospective peer review before a patient starts treatment. Mitchell et al published their experience with prospective peer review of 422 cases over 2 years and identified that 20.6% of cases were marked as having a variation, with 0.7% having a major deviation. They found that a change in contours was recommended in 10% of cases, with peer review requiring, on average, 7 minutes per case.17 Their data suggests that prospective peer review is a feasible practice and influences changes in practice.
Our institution has implemented several established processes for structured peer review, which requires the following in order to be effective: active participation from providers; a supportive and respectful environment; support from leadership to maintain dedicated time and reduced interruptions; and availability of facilities and technology to access images, electronic medical record data, planning images, and remote capabilities for off-site participants. Most time is dedicated to our weekly retrospective chart review of all new patient treatment starts, which includes participation of physicians, physics, dosimetry, and therapists. To increase consistency of practice patterns across hospitals within our integrated healthcare system, we have implemented monthly, disease-site specific, retrospective peer review. Prospective peer review efforts include all stereotactic body radiation therapy (SBRT) treatment plans and head and neck treatment plans and, most recently, review of challenging cases across hospitals within our integrated healthcare system. This includes a voluntary review of contours and dosimetry using disease-site-specific teams of experts. The ultimate goal of prospective peer review is to standardize treatment plans and establish the same quality of care throughout the enterprise. In addition, the reduction in variability potentially may reduce treatment errors through consistency.
Quality Improvement, Patient Safety in Radiation Oncology Resident Education
The Accreditation Council for Graduate Medical Education (ACGME) mandates resident and fellow participation in quality and patient safety education; however, release of the Clinical Learning Environment Review demonstrated that trainee knowledge of formal methods for patient safety reporting and analysis can be improved.18 Our department encourages resident participation in the WE Team and, in keeping in line with ACGME requirements, a resident-led quality and patient safety project is implemented within the department annually. Examples of resident-led initiatives in our department include standardization of disease-site-specific simulation request templates, creation of dosimetric score cards to standardize treatment plan evaluation, and implementation of atlas-based auto-segmentation to standardize normal tissue contouring. Encouraging education of the science and methods of quality improvement and patient safety for trainees will promote these processes in practice and lead to lasting change. Also, developing a mindset of quality improvement and safety will lead to ongoing continuous improvement as residents graduate and enter practice.
Implementing and Sustaining Change
Although these initiatives were in a large academic, tertiary care center, many of these strategies can be implemented in much smaller centers by utilizing all members in the department including physicists, dosimetrists, therapists, nurses, and administrative staff. For instance, our WE Team employs all members of the department to discuss issues and develop multidisciplinary solutions to minimize recurrence. To implement and sustain these strategies, a safety culture with a blame-free environment must be developed. With this in place, an effective incident learning and reporting system can be developed. Ford et al summarizes the key components of an incident learning system, including identifying and addressing cognitive bias, which can impede effective solutions.19 This bias includes imagining that a wrong decision is being made at that time to identify cognitive missteps, considering the opposite (ie, imagining that the opposite conclusion is correct), recalibration whereby one acknowledges that bias can calibrate thinking, and crowd wisdom.
Conclusion
Avoiding harm and providing the best care is the responsibility of the health care system. As such, quality and patient safety should be priorities, which, in turn, can be improved by a safe environment and structured system to report near misses and errors, standardization and automation of workflow, and a structured peer review process. Commitment to these processes is a collective effort on both the individual and system level.
References
- Hendee WR, Herman MG. Improving patient safety in radiation oncology. Med Phys. 2011; 38(1):78-82.
- ACR-ASTRO Practice Parameter for Radiation Oncology. Radiat Oncol. https://www.acr.org/-/media/ACR/Files/Practice-Parameters/RadOnc.pdf. Accessed July 25, 2018.
- Marks LB, Jackson M, Xie L, et al. The challenge of maximizing safety in radiation oncology. Pract Radiat Oncol. 2011;1(1):2-14.
- Abdel-Wahab M, Rosenblatt E, Holmberg O, Meghzifene A. Safety in radiation oncology: the role of international initiatives by the International Atomic Energy Agency. J Am Coll Radiol. 2011;8(11):789-794.
- Tariq MB, Meier T, Suh JH, et al. Departmental workload and physician errors in radiation oncology. J Patient Saf. 2016.
- Ezzell G, Chera B, Dicker A, et al. Common error pathways seen in the RO-ILS data that demonstrate opportunities for improving treatment safety. Pract Radiat Oncol. 2018;8(2):123-132.
- Kalapurakal JA, Zafirovski A, Smith J, et al. A comprehensive quality assurance program for personnel and procedures in radiation oncology: value of voluntary error reporting and checklists. Int J Radiat Oncol Biol Phys. 2013;86(2):241-248.
- Liszewski BE, Drodge C.S., Marchand E., et al. . A National System for Incident Reporting in Radiation Therapy: Development of a Taxonomy and Severity Classification. Int J Radiat Oncol Biol Phys. 2014;90(15).
- Hoopes DJ, Dicker AP, Eads NL, et al. RO-ILS: Radiation Oncology Incident Learning System: a report from the first year of experience. Pract Radiat Oncol. 2015;5(5):312-318.
- Chao ST, Meier T, Hugebeck B, et al. Workflow enhancement (WE) improves safety in radiation oncology: putting the WE and team together. Int J Radiat Oncol Biol Phys. 2014;89(4):765-772.
- Mazur LM, Mosaly PR, Jackson M, et al. Quantitative assessment of workload and stressors in clinical radiation oncology. Int J Radiat Oncol Biol Phys. 2012;83(5):e571-576.
- Braham DL, Richardson AL, Malik IS. Application of the WHO surgical safety checklist outside the operating theatre: medicine can learn from surgery. Clin Med (Lond). 2014;14(5):468-474.
- Meier T, Suh JH, Barrett P, et al. Presimulation procedure safety checklist/time out reduces simulation related unintended deviations. Int J Radiat Oncol Biol Phys. 2017;99(2):E559.
- Covington EL, Chen X, Younge KC, et al. Improving treatment plan evaluation with automation. J Appl Clin Med Phys. 2016;17(6):16-31.
- Dixon P, O’Sullivan B. Radiotherapy quality assurance: time for everyone to take it seriously. Eur J Cancer. 2003;39(4):423-429.
- Lefresne S, Olivotto IA, Joe H, Blood PA, Olson RA. Impact of quality assurance rounds in a Canadian radiation therapy department. Int J Radiat Oncol Biol Phys. 2013;85(3):e117-121.
- Mitchell JD, Chesnut TJ, Eastham DV, Demandante CN, Hoopes DJ. Detailed prospective peer review in a community radiation oncology clinic. Pract Radiat Oncol. 2017;7(1):50-56.
- National Report of Findings: Patient Safety. Clinical Learning Environment Review 2016; https://www.acgme.org/Portals/0/PDFs/CLER/ACGME_CLER_Patient-Safety_Digital.pdf. Accessed July 25, 2018.
- Ford EC, Evans SB. Incident learning in radiation oncology: A review. Med Phys. 2018;45(5):e100-e119.
Citation
BV M, N Y, T M, JH S, ST C. A review of strategies for optimizing workflow, quality improvement, and patient safety within radiation oncology departments. Appl Radiat Oncol. 2018;(4):8-12.
December 20, 2018