Metastases from glioblastoma disguised as a new primary malignancy
Images
Case Winner March 2016
CASE SUMMARY
A 65-year-old man with a history of glioblastoma (GBM) of the right frontotemporal lobes who was treated with radiation therapy and concurrent/adjuvant temozolomide (TMZ) had a recurrence 3 months after standard chemoradiotherapy. He was subsequently treated with bevacizumab, lomustine, and Gamma Knife (Elekta, Stockholm, Sweden) stereotactic radiosurgery (GKSRS). Following GKSRS, he was treated with NovoCure tumor treating fields (NovoTTF; NovoCure, Portsmouth, New Hampshire). Approximately 9 months later, he developed back pain, right-sided ptosis, and sinus congestion-like symptoms. Spinal computed tomography (CT) imaging showed multilevel spinal disease, and MR imaging showed lesions in the T8-10 vertebral region. Imaging of the head suggested a new paranasal sinus primary tumor, suspicious for the origin of his metastatic disease. The patient underwent a T7-8 kyphoplasty, the pathology from which showed glial fibrillary acidic protein (GFAP), epithelial membrane antigen (EMA), and CD138 positivity, which was suggestive but not definitive for metastatic GBM. He presented 1 week later with worsening sinus congestion/ptosis, and had repeat imaging of the head (see below). Body imaging showed pulmonary and hepatic lesions. The patient underwent a biopsy of his paranasal sinus disease and the result was consistent with metastatic GBM.
Because of his significant back pain, we simulated him for palliative radiation therapy to his cervical and thoracic spinal disease, as it was having the greatest impact on his quality of life. We treated his cervical disease (8 Gy × 1) and then he requested we defer the thoracic radiation therapy to another day because of discomfort from lying on the table. The next day, the treatment conditions became unsafe secondary to the patient’s inability to lie on the table and his thoracic radiation therapy was terminated. He was discharged to home with hospice and died approximately 3 weeks later.
IMAGING FINDINGS
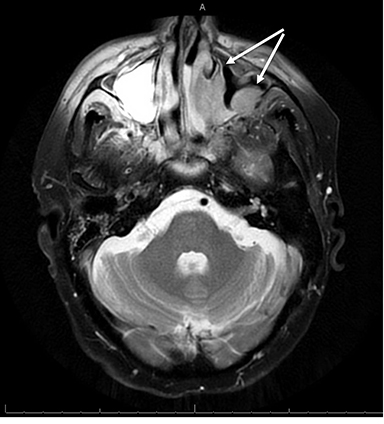
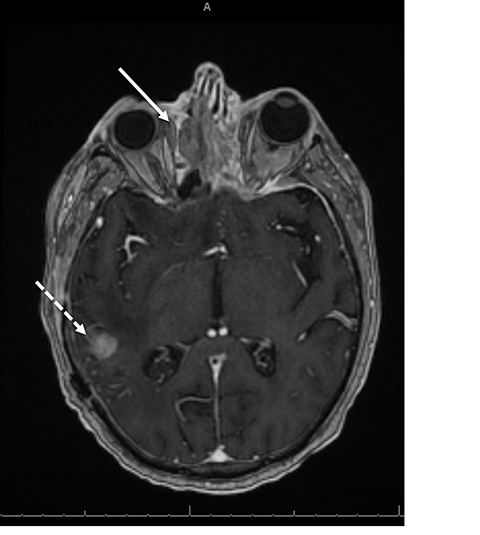
An MRI of the head showed destructive changes in the paranasal sinuses with destruction of the left maxillary sinus and extension into the left retroantral fat, pterygopalatine fossa, and hard palate. The left lamina papyracea and left orbital roof were being invaded by a soft tissue mass in the left orbit measuring 2.6 × 0.9 cm, which engulfed the superior rectus, oblique, and medial rectus muscles (Figures 1 and 2).
DIAGNOSIS
The patient was diagnosed with widely metastatic glioblastoma. The initial suspicion was that he had developed a metastatic paranasal sinus primary tumor, which was disproved by his biopsy.
DISCUSSION
GBM is the most common histology of malignant primary brain tumors in adults.1 Despite advances in surgical, medical, and radiation therapies, the mortalities of GBM remain high, with a median survival ranging between 40 and 70 weeks,2 although recent clinical trial data has shown promise for improving outcomes with the addition of NovoTTF.3 The majority of GBM recur locally, and distant metastasis is rare, estimated to occur in < 2% of patients.4 In spite of infrequent clinical presentation of distant metastases, circulating GBM cells have been detected in up to 20.6% of patients,5 which may lead to metastases to the lymphatics, lungs, bone, liver, and other organs.6
CONCLUSION
A diagnosis of GBM is a grim diagnosis from the start. When patients survive long enough to develop metastatic disease, however, the median time from detection of metastatic disease to death has been reported to be as short as 1.5 months.6 Although data is limited, it has been suggested that metastases to the liver have a lesser impact on survival than metastases to the lung.7 The treatment of choice for asymptomatic patients is systemic therapy, although when quality of life is affected by disease burden, surgical intervention or focal radiation therapy can be considered, as was the case with our patient.
REFERENCES
- Ostrom QT, Gittleman H, Liao P, et al. CBTRUS statistical report: primary brain and central nervous system tumors diagnosed in the United States in 2007–2011. Neuro Oncol. 2014;16: iv1-iv63.
- Thakkar JP, Dolecek TA, Horbinski C, et al. Epidemiologic and molecular prognostic review of glioblastoma. Cancer Epidemiol Biomarkers Prev. 2014;23:1985-1996.
- Stupp R, Taillibert S, Kanner A, et al. Tumor treating fields (TTFields): a novel treatment modality added to standard chemo- and radiotherapy in newly diagnosed glioblas
- toma—First report of the full dataset of the EF14 randomized phase III trial. J Clin Oncol. 33,2015(suppl; abstr 2000).
- Khattab MH, Marciscano AE, Lo SS, et al. Antiangiogenic therapies and extracranial metastasis in glioblastoma: a case report and review of the literature. Case Rep Oncol Med. 2015;2015:431819.
- Muller C, Holtschmidt J, Auer M, et al. Hematogenous dissemination of glioblastoma multiforme. Sci Transl Med. 2014;6(247):247ra101.
- Lun M, Lok E, Gautam S, et al. The natural history of extracranial metastasis from glioblastoma multiforme. J Neurooncol. 2011;105(2):261-273.
- Fonkem E, Lun M, Wong ET. Rare phenomenon of extracranial metastasis of glioblastoma. J Clin Oncol. 2011;29(34):4594-4595.
Citation
JL R, ZD H, JC F. Metastases from glioblastoma disguised as a new primary malignancy. Appl Radiat Oncol. 2016;(1):26-27.
March 7, 2016