Minimally invasive hysterectomy for uterine cancer: A radiation oncologist’s perspective
Images
Endometrial cancer is the most commonly diagnosed gynecological malignancy in the United States, with 47,130 estimated new cases in 2012.1 Hysterectomy with bilateral salpingo-oophorectomy, with or without pelvic or para-aortic lymphadenectomy, is the standard staging procedure for patients with endometrial cancer.2
Traditionally, endometrial cancer has been surgically managed with laparotomy through a large vertical incision. More recently, robotic-assisted laparoscopic hysterectomy (da Vinci System, Intuitive Surgical System, Inc., Sunnyvale, CA) has been adopted for treatment of endometrial cancer in many centers all over the world. Recent studies reported a reduction in perioperative complications and shorter hospital stays with quicker recovery for laparoscopic approaches compared to total abdominal hysterectomy.3-7
However, with the increased use of laparoscopic, including robotic-assisted, hysterectomies, there appears to be an increased rate of vaginal-cuff dehiscence, a rare complication after hysterectomy. The rate of this complication is relatively higher after robotic-assisted hysterectomy, reaching up to 4.1%8 compared to < 1% following total abdominal hysterectomy.9
The radiation oncologist’s perspective
While surgical staging alone is curative in most of the patients with early-stage endometrial carcinoma, selected patients with an adverse prognostic feature, eg, high tumor grade, deep myometrial invasion, and nonendometrioid histology, will benefit from adjuvant radiation therapy following hysterectomy. Two major prospective, randomized studies showed that adjuvant radiation treatment after hysterectomy resulted in a significant reduction in locoregional recurrence.10-11
The use of adjuvant vaginal-cuff brachytherapy for patients with endometrial cancer is effective in reducing vaginal-vault recurrence, which is the most common site of recurrence after hysterectomy in patients with endometrial cancer. In a prospective randomized study (PORTEC-2), vaginal-cuff brachytherapy was compared to pelvic external beam radiation treatment (EBRT) in regards to efficacy in reducing vaginal-cuff recurrence as well as health-related quality of life. The estimated 5-year rate of vaginal recurrence was only 1.8% after vaginal-cuff brachytherapy.12
With the increased utilization of vaginal brachytherapy as an effective adjuvant treatment following hysterectomy,13 together with the increased utilization of minimally invasive hysterectomy for patients with endometrial cancer, we sought to discuss our perspectives in regard to the potential challenge of an increased rate of vaginal-cuff dehiscence after a robotically-assisted hysterectomy for those patients who will require adjuvant vaginal-cuff brachytherapy.
The relative increased rate of vaginal-cuff dehiscence is attributed to a variety of reasons, including the use of electrocautery for colpotomy, the suturing technique used, and the magnification view causing suture bites to be smaller than desired. Predisposing factors for vaginal-cuff dehiscence include poor wound healing, excessive pressure at the vaginal vault, eg, sexual intercourse,14 and vaginal instrumentation, eg, the insertion of a vaginal cylinder for vaginal brachytherapy.15 Other proposed risk factors for vaginal-cuff dehiscence include poor surgical technique, smoking, use of the Valsalva maneuver, postoperative infection, hematoma, steroid use, connective tissue disease, vaginal trauma/rape, use of vaginal dilator, diabetes mellitus, and chronic constipation.16-18
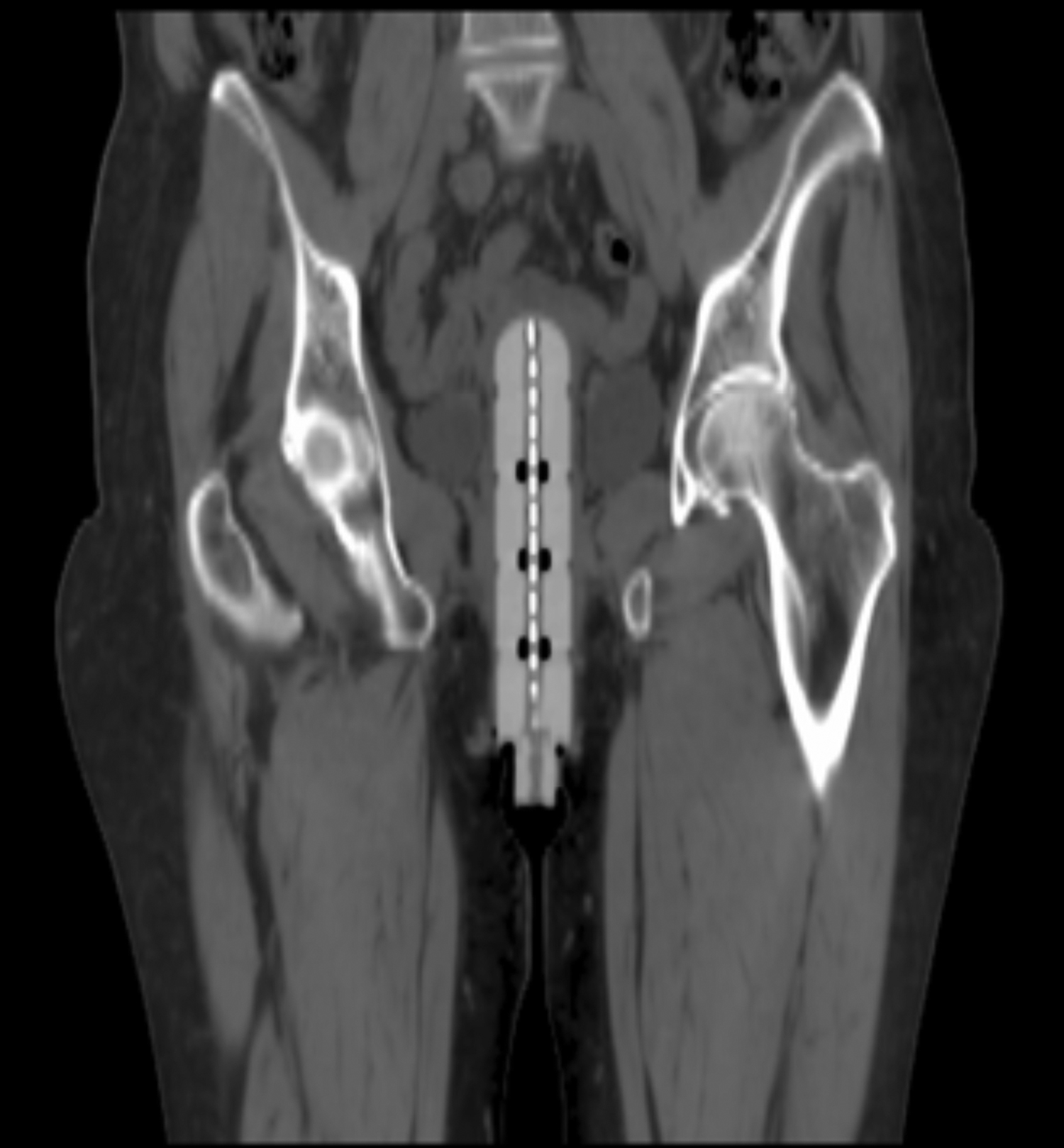
While there is only one case report to date for patients with vaginal dehiscence as a result of vaginal-cuff brachytherapy, we think this complication is under reported. We have recently diagnosed a patient with vaginal-cuff dehiscence as a result of vaginal-cuff brachytherapy. A 62-year-old female underwent robotic-assisted laparoscopic hysterectomy with bilateral salpingo-oophorectomy for FIGO 2009 stage IB endometrioid adenocarcinoma, FIGO grade 1. Based on a multidisciplinary tumor conference, it was recommended to treat her with adjuvant vaginal-cuff brachytherapy. She presented for computed tomography (CT) simulation for vaginal-brachytherapy treatment planning approximately 9 weeks after her hysterectomy. During simulation, the vaginal cylinder was noted to abnormally project high into the pelvis (Figure 1). On speculum examination, there was evidence of complete vaginal-cuff dehiscence. She underwent surgical closure of the vaginal cuff on the same day.
Radiation oncologists should be aware of the very low risk of vaginal-cuff dehiscence and take steps prevent and detect the condition as early as possible. At the time of the brachytherapy simulation, it can be useful to perform careful speculum and manual examinations of the vaginal cuff for findings of vaginal-cuff dehiscence. The appropriate size of the vaginal cylinder should be selected. The location of the vaginal cylinder should be radiologically verified with each application to rule out abnormal positioning of the cylinder.
Vaginal-cuff dehiscence should be ruled out if the vaginal cylinder projects abnormally deep in the pelvis. To reduce the risk of dehiscence during insertion of the vaginal cylinder, it is helpful to avoid high pressure on the vaginal cuff. After the procedure, one should inspect the vaginal cylinder for any abnormal blood or clear vaginal fluid that could suggest dehiscence. On the other hand, this very rare complication can be prevented by initiating vaginal brachytherapy no sooner than 6 weeks after a hysterectomy to allow adequate healing time.19 However, delaying the start of adjuvant radiation treatment > 9 weeks after a hysterectomy may be associated with increased risk of tumor recurrence.20
Conclusion
Vaginal-cuff dehiscence is an unusual complication of hysterectomy. With the increased use of laparoscopic, robotic-assisted approaches, there appears to be an increased rate of vaginal-cuff dehiscence. In addition, there is an increased use of adjuvant vaginal brachytherapy for treatment of endometrial cancer. Although vaginal-cuff dehiscence is still very rare after vaginal-cuff brachytherapy, patients should be counseled about this rare treatment-related complication. Early identification and urgent management of this complication is recommended.
References
- Siegel R, Naishadham D, and Jemal A, Cancer Statistics, 2012. CA Cancer J Clin. 2012;62:10-29.
- Pecorelli S. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. Int J Gynaecol Obstet. 2009;105:103.
- Ribeiro SC, Ribeiro RM, Santos NC, et al. A randomized study of total abdominal, vaginal and laparoscopic hysterectomy. Int J Gynaecol Obstet. 2003;83:37-43.
- Cho Y-H, Kim D-Y, Kim J-H, et al. Laparoscopic management of early uterine cancer: 10-year experience in Asan Medical Center. Gynecol Oncol. 2007;106:585-590.
- Bell MC, Torgenson J, Seshadri-Kreaden U, et al. Comparison of outcomes and cost for endometrial cancer staging via traditional laparotomy, standard laparoscopy and robotic techniques. Gynecol Oncol. 2008;111:407-411.
- Boggess JF, Gehrig PA, Cantrell L, et al. A comparative study of 3 surgical methods for hysterectomy with staging for endometrial cancer: Robotic assistance, laparoscopy, laparotomy. Am J Obstet Gynecol. 2008;199:360.
- DeNardis SA, Holloway RW, Bigsby IV GE, et al. Robotically assisted laparoscopic hysterectomy versus total abdominal hysterectomy and lymphadenectomy for endometrial cancer. Gynecol Oncol. 2008;111:412-417.
- Kho R, Akl M, Cornella J, et al. Incidence and characteristics of patients with vaginal cuff dehiscence after robotic procedures. Obstet Gynecol. 2009;114:231-235.
- Croak A, Gebhart J, Klingele C, et al. Characteristics of patients with vaginal rupture and evisceration. Obstet Gynecol. 2004;103:572-576.
- Creutzberg CL, van Putten WL, Koper PC Lybeert ML, et al. Surgery and postoperative radiotherapy versus surgery alone for patients with stage-1 endometrial carcinoma: Multicentre randomised trial. PORTEC study group. Post operative radiation therapy in endometrial carcinoma. Lancet. 2000;355:1404-1411.
- Keys HM, Roberts JA, Brunetto VL, et al. A phase III trial of surgery with or without adjunctive external pelvic radiation therapy in intermediate risk endometrial adenocarcinoma: A Gynecologic Oncology Group study. Gynecol Oncol. 2004;92:744-751.
- Nout R, Smit V, Putter H, et al. Vaginal brachytherapy versus pelvic external beam radiotherapy for patients with endometrial cancer of high-intermediate risk (PORTEC-2): An open-label, non-inferiority, randomised trial. Lancet. 2010;375:816-823.
- Patel M, Cote M, Ali-Fehmi R, et al. Trends in the utilization of adjuvant vaginal cuff brachytherapy and/or external beam radiation treatment in stage I and II endometrial cancer: A surveillance, epidemiology, and end-results study. Int J Radiat Oncol Biol Phys. 2012;83:178-184.
- Kalu E, Fakokunde A, Evans-Jones J. Postcoital vault dehiscence and instestinal prolapse following abdominal hysterectomy. J Obstet Gynaecol. 2006;26:74-75.
- Albuquerque K, Shah K and Potkul R. Vaginal cuff dehiscence after intracavitary brachytherapy for endometrial cancer. J Contemp Brachytherapy. 2012:111-112.
- Agdi M, Al-Ghafri W, Antolin R, et al. Vaginal vault dehiscence after hysterectomy. J Minim Invasive Gynecol. 2009;16:313-317.
- Ceccaroni M, Beretta R, Malzoni M, et al. Vaginal cuff dehiscence after hysterectomy: A multicenter retrospective study. Eur J Obstet Gynecol Reprod Biol. 2011;158:308-313.
- Somkuti S, Vieta P, Daugherty J, et al. Transvaginal evisceration after hysterectomy in premenopausal women: A presentation of three cases. Am J Obstet Gynecol. 1994;171: 567-568.
- Kirsner R, Eaglstein W. The wound healing process. Dermatol Clin. 1993;11:629-640.
- Elshaikh MA, Cattaneo II R, Jacobson G, et al. Interval between hysterectomy and start of radiation treatment is predictive of recurrence in patients with endometrial carcinoma. A single Institution experience. Int J Radiat Oncol Biol Physics. 2012;84(3S, supplement):S97.