Upfront Surgery With Adjuvant RT Vs Chemoradiation in HPV-Mediated Oropharyngeal Cancer in Intermediate-Risk Patients
Images

Abstract
Background: We conducted a multi-institutional retrospective review of patients with HPV-mediated oropharyngeal squamous cell carcinoma (HPV-SCC) to compare outcomes for upfront oncologic surgery plus adjuvant radiation therapy (RT) or chemoradiation therapy.
Methods: We analyzed 281 patients from two institutions treated from 2010 to 2017. The primary outcome was event-free survival (EFS). Secondary outcomes were overall survival (OS), locoregional control and major complications. Univariate (UVA) and multivariate (MVA) Cox proportional hazards models were done, and Kaplan-Meier survival curves generated.
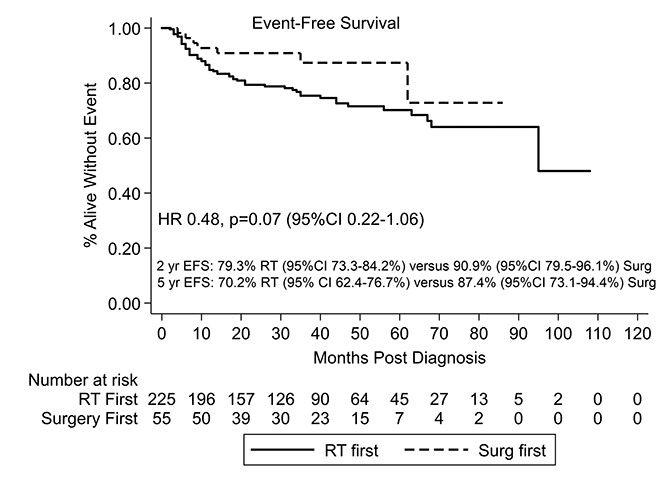
Results: There were 55 surgery and 226 RT patients, median follow-up 37 months. There were fewer locoregional failures (0% vs 11%, P = 0.04) but more major complications (18% vs 11%, P < 0.01) for surgery patients. Adjuvant chemoradiation therapy was utilized in 44%. On UVA there was a trend for improved EFS in the surgery group (HR 0.48, P = 0.07), which did not persist on MVA (HR 1.07, P = 0.91).
Conclusion: Upfront surgery did not improve EFS or OS. Local control improved, with more major complications.
The incidence of human-papillomavirus-related squamous cell carcinoma (HPV-SCC) of the oropharynx is increasing internationally.1-3 Fortunately, the prognosis with treatment is favorable, but at the cost of both acute and late toxicity.3-6 Efforts are underway to preserve and improve survival outcomes while decreasing toxicity with upfront surgical resection,7-9 decreasing definitive radiation therapy (RT) doses/volume, or eliminating chemotherapy10 in certain patients.
Newer surgical techniques are thought to have significantly lower toxicity compared with prior techniques,11-13 with potential to eliminate RT in lowest-risk patients, decrease the adjuvant RT dose in intermediate-risk patients (T3/T4 tumors, two or more positive lymph nodes, close margins, perineural invasion [PNI], lymphovascular space invasion [LVSI]), eliminate chemotherapy in high-risk patients (positive margins, extranodal extension), and possibly improve survival outcomes for highest-risk patients. When compared with results from previous RT trials,14 the toxicity profile appears to be improved, although such comparisons between datasets are problematic.
Until recently, no randomized trial had been published comparing outcomes between upfront treatment modality, whether surgery or RT; only a few retrospective series have described outcomes between these patients.15,16 Despite the paucity of data comparing the effectiveness and/or toxicity of either definitive treatment, the incidence of upfront surgical resection has increased significantly (56% to 82% from 2004 to 2015) in facilities that report to the National Cancer Database (NCDB).17
Given this lack of data regarding the most appropriate primary treatment for patients with HPV-SCC, we sought to compare upfront surgical resection vs RT or chemoradiation therapy in a multi-institutional retrospective review.
Methods
Patients treated with RT at Intermountain Healthcare and Huntsman Cancer Hospital from 2010 to 2017 for nonmetastatic HPV-SCC were included in this study. These are independent institutions in the Salt Lake area with independently practicing physicians, and both have an average of two to three head and neck (H&N) radiation oncologists, three H&N fellowship-trained surgeons, and one medical oncologist. This study was exempt from both centers’ institutional review boards after initial review (IRB#1051068 and #00012307). To be included, patients could not have another concurrent cancer at diagnosis and had to be treated with curative intent. For primary RT, this required a dose of at least 66 Gray (Gy) to the primary tumor, and treatment of the bilateral neck (or unilateral neck for well-lateralized tonsillar primaries). For surgical patients, this was defined either as a transoral robotic surgery (TORS) or wide local excision with neck dissection of at least the ipsilateral levels II-IV, followed by adjuvant RT. Generally, patients with positive surgical margins or extranodal extension received adjuvant chemoradiation therapy. Occasionally patients with PNI, extensive nodal disease, or other high-risk factors received adjuvant chemoradiation therapy at the discretion of the treating physicians.
Patient data collected included demographic factors: age, gender, performance status, and smoking status (current, former 10 pack-years, former < 10 pack-years, and nonsmoker). Clinical tumor factors included: p16 status; primary tumor size; primary tumor location; location of involved lymph nodes (ipsilateral or bilateral); and the American Joint Committee on Cancer (AJCC) 7th and 8th edition tumor (T), node (N), and overall group stage. Treatment factors collected included: upfront treatment (oncologic surgery or RT), RT dose, and whether systemic therapy was given and, if so, type. In patients who underwent upfront surgery, data collected included pathologic tumor size, T stage (8th edition), PNI, LVSI, margin status, number of nodes involved, pathologic N stage (8th edition), whether nodes were ipsilateral or bilateral, and whether extranodal extension (ENE) was present. Time from surgical resection to the start of RT was also collected. Clinical outcomes collected included time from diagnosis to last follow-up, vital status (alive or dead), cause of death if applicable, local recurrence status, distant metastases status, time to local recurrence or distant metastases, salvage method if applicable, and major complications. Major complications included feeding tube dependence > one year, osteoradionecrosis, carotid injury requiring intervention or causing death, spinal cord injury, severe lymphedema requiring ongoing therapy or limiting quality of life, or other major event thought to be related to cancer treatment as documented in the medical record.
Differences between the demographic, clinical, treatment, and outcome factors between treatment groups were compared using chi-square analysis. The primary outcome was event-free survival (EFS), which included death from any cause, locoregional recurrence, or distant recurrences. Secondary outcomes included OS, locoregional failure rate, and major complication rates. Both EFS and OS were examined using Cox-proportional hazards modeling via univariate analysis (UVA) followed by multivariate analysis (MVA). Demographic, clinical, and treatment factors with a P-value of < 0.2 were included in the multivariate model and Kaplan-Meier curves were then generated.18 A P-value of < 0.05 was required for significance. Patients were then stratified into a low-risk group (LR) and a high-risk group (HR) similar to the stratification from RTOG 0129.19 Patients in the LR group were AJCC 7th edition T0-2, N0-2a, with any smoking status. There were not enough nonsmokers/< 10 pack-year smokers in the low T/N stage RT group to lend statistical significance, so smoking status was not included for low-risk stratification. The HR patients had more advanced disease (N2b-3) and either were current smokers or had a smoking history > 10 pack-years. In these patients, EFS and OS were also examined on UVA.
Results
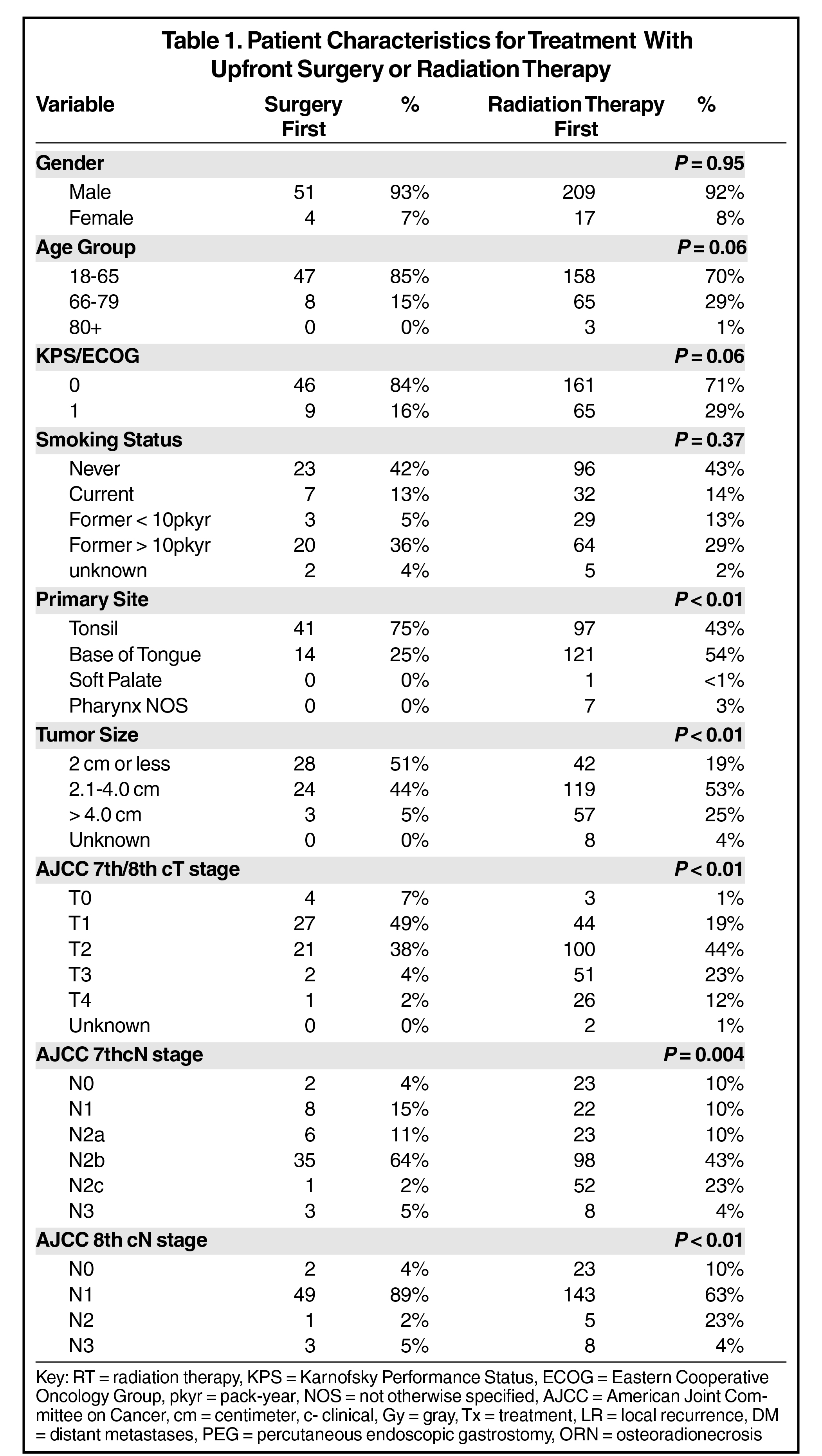
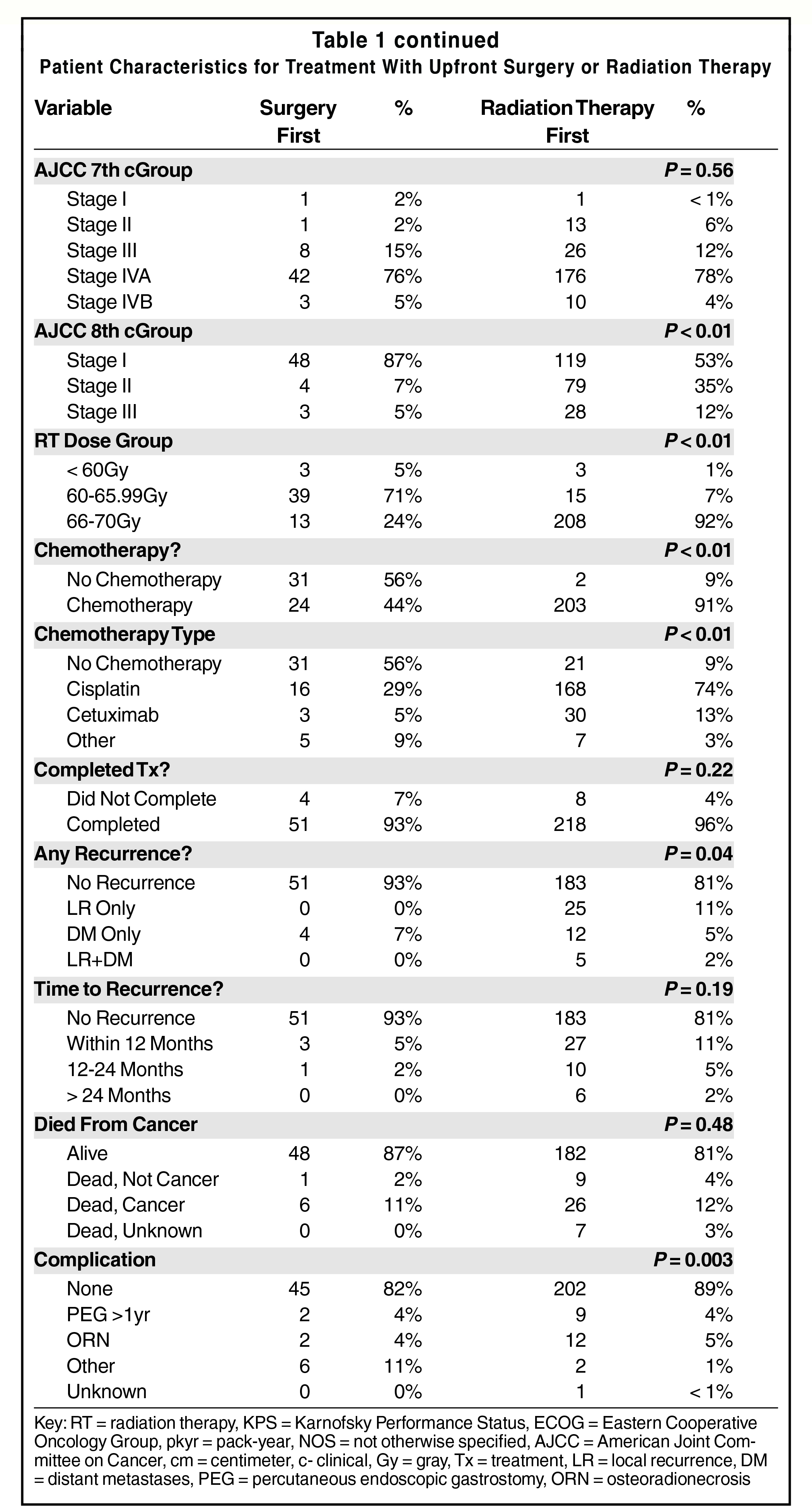
There were 281 patients who met inclusion criteria for this study, 55 of whom underwent oncologic surgery as their primary treatment and 226 of whom underwent primary RT. Median age was 60 and median follow-up time for all patients was 37 months, 37 for the RT group and 33 for the surgery group. The groups were well-balanced in terms of gender and smoking status (Table 1). There was a strong trend toward older age in the RT group (30% over 65 vs 15%, P = 0.06) and poorer performance status (29% ECOG 1 vs 16%, P = 0.06) (see Table 1). Base of tongue location was more common in the RT group (54% vs 25%, P < 0.01), as were tumors > 4 cm (25% vs 5%, P < 0.01) with subsequently more advanced AJCC 7th/8th edition T stage (64% T0-T2 vs 94%, P > 0.01). RT patients also had more advanced nodal disease, with N2c-N3 (7th edition) disease accounting for 27% vs 7% of surgical patients (P = 0.004). In patients who underwent upfront surgical resection, all underwent postoperative adjuvant RT, and 24% of patients underwent high-dose RT (66-70 Gy) (Table 1). Of the surgical patients, 16% had positive margins, 24% had extranodal extension, and 44% underwent adjuvant chemoradiation therapy. All patients started RT within 8 weeks of surgery. Rates of treatment completion did not differ between the two groups. Surgical patients were less likely to have local recurrences (0% vs 11%, P = 0.04), but more likely to have major complications (18% vs 11%, P = 0.003), see Table 1. Feeding-tube dependence > 1 year and osteoradionecrosis (ORN) rates were comparable (~ 4%), but the rates of carotid, spinal cord, and soft-tissue injury were higher in the surgery arm (11% vs 1%, P = 0.003), see Table 1. Of that 11%, 5 out of 6 patients received adjuvant RT alone and 2 out of 6 received curative high-dose RT.
On UVA, there was a trend toward improved EFS with surgery compared to RT (HR 0.48, P = 0.07), which was lost on MVA (HR 1.07, P = 0.91) (see Table 2, Figure 1). Factors associated with worsened EFS included being a former smoker of < 10 pack-years compared with a never smoker (HR 2.49, P = 0.02) and cetuximab compared with no systemic therapy (HR 6.13, P = 0.02). There was a trend for decreased EFS for age 80+ compared with age 18 to 65 (HR 6.45, P = 0.09), former smokers > 10 pack-years compared with never smokers (HR 1.86, P = 0.06), soft palate site compared with tonsil (HR 7.25, P = 0.08), cN3 stage compared with cN1 (HR 2.50, P = 0.08), and cisplatin compared with no chemotherapy (HR 3.15, P = 0.09).
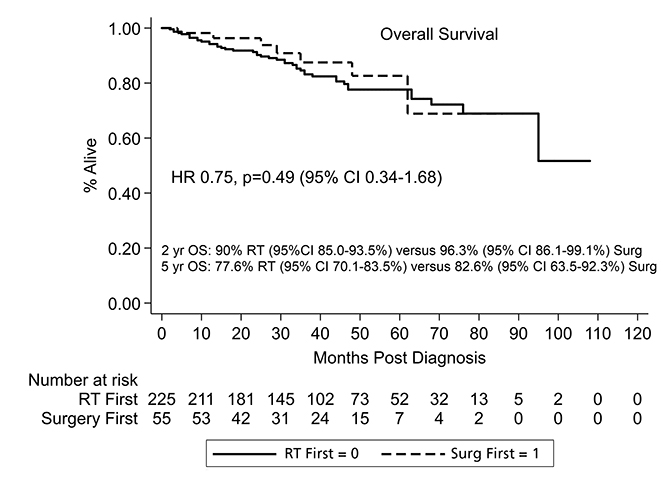
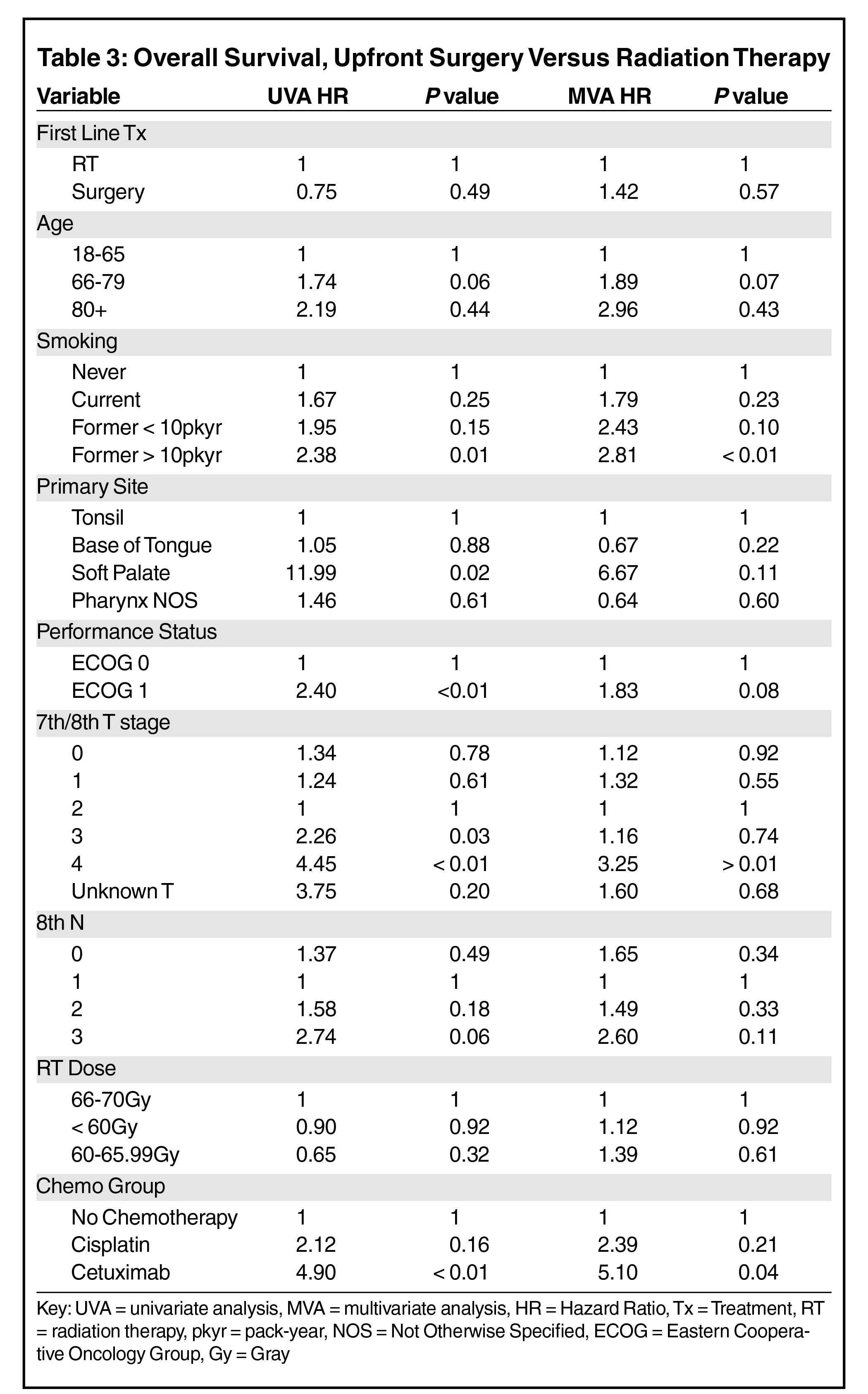
With respect to OS, upfront resection did not affect survival on either univariate (HR 0.75, P = 0.49) or multivariate analysis (HR 1.42, P = 0.57). There was a trend toward decreased survival for patients aged 66 to 79 compared with 18 to 65 (HR 1.89 P = 0.07) and ECOG 1 performance status (HR 1.83, P = 0.08) compared with ECOG 0. There was significant detriment for former >10 pack-year smokers (Table 3, Figure 2) compared with nonsmokers (HR 2.81, P < 0.01), patients with T4 disease compared with T2 (HR 3.25, P > 0.01), and cetuximab therapy compared with no chemotherapy (HR 5.10, P = 0.04).
On subgroup analysis, there were 169 low-risk patients (cT0-T2, cN0-1 AJCC 8th edition). Neither EFS (HR 0.91, P = 0.84) nor OS (HR 1.62, P = 0.35) were affected by the method of upfront treatment on UVA. Of low-risk surgery patients, 40% underwent adjuvant chemoradiation therapy, 22% underwent high-dose RT, 18% had positive margins, and 10% had ENE. There remained an 11% higher complication rate in surgery patients (P = 0.02) with a trend toward improved local control (0% local recurrences vs 8%, P = 0.06). There were 88 high-risk patients (cN2b-3 7th edition, >10 pack-year or current smokers). Neither EFS (HR 0.95, P = 0.92) nor OS (HR 1.27, P = 0.62) were affected by upfront treatment on UVA. Of high-risk surgery patients, 55% underwent adjuvant chemoradiation therapy and 35% underwent high-dose RT. There was a 15% higher rate of major complications for upfront surgery (25% vs 10%, P = 0.02) with a 15% decrease in local recurrences (P = 0.02).
Discussion
In this study, patients with HPV-SCC of the oropharynx, initial surgical resection was not associated with improved EFS or OS compared to upfront RT. Surgery was associated with a small decrease in rate of local recurrences at the expense of increased rates of major complications, particularly injury to the ipsilateral carotid artery, spinal cord, or skin and soft tissue. Of patients who started with surgery, nearly half received trimodality therapy (surgery, RT, chemotherapy) and nearly a quarter received curative-dose RT. On subgroup analysis, neither the low- nor the high-risk patients benefitted from upfront surgical resection and in the high-risk patients, upfront surgery was associated with a 25% rate of major complications.
Although there was an initial trend toward improved EFS with initial resection, when other factors were considered on MVA, such as stage and performance status, this trend disappeared. The lack of a trend for OS between groups combined with the difference in rates of locoregional control on chi-square analysis suggest that the improvement in EFS was likely driven by locoregional control and that these patients are highly salvageable. In fact, of the 25 patients who failed locally, 70% of them were surgically salvaged. The locoregional control difference was likely secondary to more advanced stage patients in the RT group. Notably, there was no improvement in survival even for the highest-risk subgroup (former smokers with advanced nodal disease), for whom treatment escalation may have been beneficial. The lack of improvement in survival is informative and consistent with previously published retrospective data16 and a recently reported randomized trial,20 although survival based on upfront treatment was not the primary outcome in either of these studies. The lack of survival benefit was also shown in a meta-analysis of seven published studies that compared both modalities, but these data are limited by poor quality data in the included studies.15 A recently published NCDB report also found that survival with upfront surgery was not improved with HPV-SCC, but was improved in HPV-negative disease.21 Interestingly, a recently presented study of 96 patients in Japan found that patients who were locally advanced but resectable had a trend toward improved survival with upfront surgery or induction chemotherapy followed by surgery,22 something that could not be confirmed in this retrospective study.
The difference in rates of major complications between the two modalities was surprising, especially since more than half of the upfront surgery patients did not receive chemotherapy and only a quarter of them received high-dose RT. Even more surprising was the type of complications these patients suffered (carotid, spinal cord, lymphedema). Similarly, a recently published series of 267 patients treated with upfront surgery over 8 years found that major (ie, PEG tube dependence and tracheostomy) complication rates were low, but other meaningful outcomes, such as aspiration of thin liquids (17% with adjuvant RT, 33% with adjuvant chemoradiation), difficulty with understandable speech (~40%), and diet limited to soft foods (27% to 46%), were present in a significant proportion of patients.23 This lack of improvement in toxicity outcomes has also been seen in the more commonly discussed toxicities, as upfront surgery was also associated with a nonclinically meaningful worsened swallowing function in the ORATOR trial, although rates of PEG tube dependence were low in both arms. The trial found a clinically meaningful decline in global and emotional functioning at one year in the surgical arm and a trend toward decreased ability to tolerate a normal diet without restrictions at one year (84% vs 100%, P = 0.055). Toxicities also differed in quality between groups. Conversely, the same study of 96 locally advanced HPV-SCC patients in Japan also found that those who underwent upfront surgical resection had less aspiration pneumonia and need for supplemental nutrition than patients treated with upfront RT.22 These studies suggest the importance of considering a wide range and degree of toxicity and complications when comparing data from primary modalities. As we await the final manuscripts for both phase II de-escalation trials (HN-002 and E3311) to better detail acute and long-term toxicities, this data serves as an important reminder that comparing these modalities is not comparing “apples to apples.” In other words, toxicities between treatments may not be classified as better, just different.
It is also important to recognize that the purpose of this study was not to assess whether upfront surgical resection could completely negate the need for adjuvant therapy in the lowest-risk patients (ie, T1-T2 primaries, 7th edition N0-1, no PNI/LVSI), as approximately 70% of surgical patients in this study had at least N2b disease. In this largely intermediate risk cohort, 44% of surgery patients underwent chemoradiation therapy (trimodality) and a quarter received high-dose treatment. This is consistent with other retrospective data that included lower-risk patients.23-25 On ECOG 3311, which assessed the role of surgery in the de-escalation of treatment for HPV-SCC based on pathologic criteria after surgery, approximately 1/3 of patients met the high-risk criteria after surgery (positive margins or > 1mm ENE) and received tri-modality therapy despite a rigorous credentialing and review process.26 Patients fared slightly better on the ORATOR trial,20 which compared quality-of-life outcomes after either surgery or RT as initial treatment, with 24% of patients requiring adjuvant chemoradiation therapy. Taken together, these data would suggest that upstaging remains a significant risk for surgical patients even with aggressive staging, with the risk increasing with expanding disease burden on presentation.
This study and others like it may one day become obsolete if de-escalation becomes standard of care, whether through de-escalated primary or adjuvant RT or surgery. However, this study and others like it should serve as a source of caution for de-escalation: Five-year overall survival was only 77% to 82% in a (relatively) young cohort with supposedly favorable disease biology, with most deaths due to cancer progression. While these numbers are excellent compared with more aggressive locally confined cancers (pancreas, glioblastoma), they are still not above 90%. The results of HN-002, a phase II trial that examined the role for reduced-dose RT +/- chemotherapy, recently found that 60 Gy plus chemotherapy may be an acceptable de-escalation option for cancer control; however, combining dose reduction with omission of chemotherapy was not.27 The 2-plus year survival rate for the RT plus chemotherapy group was excellent (90%), as were the survival rates on E3311 (93% to 95%). Although the vast majority of patients will face recurrence in the first two years, longer follow-up is needed from both a survival and toxicity standpoint for both of these trials. Certainly, RTOG 1016 seemed to urge caution on the replacement of cisplatin with cetuximab.28
The major limitation in this retrospective study was that only major complications, such as ORN, PEG tube dependence, and other major injuries, were recorded. These events were fortunately rare, but do not adequately capture a patient’s quality of life after treatment. Xerostomia, dysgeusia, trismus, dysarthria, and inability to tolerate a normal diet may not be so severe to require supplemental nutrition or render the patient without understandable speech, but can be quite limiting. Finally, although performance status was included as a part of this study, comorbidity scores were not. This is specifically relevant to the decision on whether to use systemic therapy and which particular agent. Cetuximab was associated with a significantly increased risk of death in this study, and several of these patients were given cetuximab on RTOG 1016, but several of them were also likely given cetuximab due to medical comorbidities or concern for poor tolerance of cisplatin. Despite these limitations, retrospective data continue to play an important role when comparing surgery and RT as primary treatment options, as those trials can be difficult to fully accrue. This has certainly been seen in the early stage lung cancer setting, and will likely be an issue for the ongoing ORATOR2 trial.
Conclusion
In this retrospective study, surgical resection did not improve survival outcomes. Upfront resection was associated with a lower local recurrence rate at the expense of a higher major complication rate. Subgroup analysis failed to show an effect of surgery (other than the increased complication rate) for either high- or low-risk patients. As we (cautiously) move into an era of de-escalated therapy, a wider range of toxicities and risks should be considered when choosing a primary treatment modality.
References
- Chaturvedi AK, Anderson WF, Lortet-Tieulent J, et al. Worldwide trends in incidence rates for oral cavity and oropharyngeal cancers J Clin Oncol. 2013;31(36):4550-4559.
- Chaturvedi AK, Engels EA, Pfeiffer RM, et al. Human papillomavirus and rising oropharyngeal cancer incidence in the United States. J Clin Oncol. 2011;29(32):4294-4301.
- American Cancer Society. Key Statistics for Oral Cavity and Oropharyngeal Cancers. Accessed August 15, 2019. https://www.cancer.org/cancer/oral-cavity-and-oropharyngeal-cancer/about/key-statistics.html
- Ang KK, Harris J, Wheeler R, et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N Engl J Med. 2010;363:24-35.
- Fakhry C, Westra WH, Li S, et al. Improved survival of patients with human papillomavirus-positive head and neck squamous cell carcinoma in a prospective clinical trial. J Natl Cancer Inst. 2008;100:261-269.
- Dayyani F, Etzel CJ, Liu M, et al. Meta-analysis of the impact of human papillomavirus (HPV) on cancer risk and overall survival in head and neck squamous cell carcinomas (HNSCC). Head Neck Oncol. 2010;2:15. doi: 10.1186/1758-3284-2-15
- Post Operative Adjuvant Therapy De-intensification Trial for Human Papillomavirus-related, p16+ Oropharynx Cancer (ADEPT). Accessed August 15, 2019. https://www.clinicaltrials.gov/ct2/show/NCT01687413.
- Transoral Surgery Followed by Low-Dose or Standard-Dose Radiation Therapy With or Without Chemotherapy in Treating Patients With HPV Positive Stage III-IVA Oropharyngeal Cancer (ECOG 3311). Accessed August 15, 2019. https://www.clinicaltrials.gov/ct2/show/NCT01898494
- Post-operative Adjuvant Treatment for HPV-positive Tumors (PATHOS). Accessed August 15, 2019. https://www.clinicaltrials.gov/ct2/show/NCT02215265.
- Reduced-Dose Intensity-Modulated Radiation Therapy With or Without Cisplatin in Treating Patients With Advanced Oropharyngeal Cancer. Accessed August 15, 2019. https://www.clinicaltrials.gov/ct2/show/NCT02254278.
- Hutcheson KA, Holsinger FC, Kupferman ME, et al. Functional outcomes after TORS for oropharyngeal cancer: a systematic review. Eur Arch Otorhinolaryngal. 2015;272:463-471.
- Haughey BH, Hinni ML, Salassa JR, et al. Transoral laser microsurgery as primary treatment for advanced-stage oropharyngeal cancer: A United States multicenter study. Head Neck. 2011;33:1683-1694.
- Canis M, Martin A, Kron M, et al.Results of transoral laser microsurgery in 102 patients with squamous cell carcinoma of the tonsil. Eur Arch Otorhinolaryngal. 2013;270:2299-2306.
- Machtay M, Moughan J, Trotti A, et al. Factors associated with severe late toxicity after concurrent chemoradiation for locally advanced head and neck cancer: an RTOG analysis. J Clin Oncol. 2008;26:3582-3589.
- Sinha P, Karadaghy OA, Doering, MM, et al. Survival for HPV-positive oropharyngeal squamous cell carcinoma with surgical versus non-surgical treatment approach: a systematic review and meta-analysis. Oral Oncol. 2018;86:121-131. doi: 10.1016/j.oraloncology.2018. 09.018.
- Vawda N, Banerjee RN, Debenham BJ. Impact of smoking on outcomes of HPV-related oropharyngeal cancer treated with primary radiation or surgery. IJROBP. 2019;103(5):1125-1131. doi: 10.1016/j.ijrobp.2018.11.046
- Cracchio JR, Baxi SS, Morris LG, et al. Increase in primary surgical treatment of T1 and T2 oropharyngeal squamous cell carcinoma and rates of adverse pathologic features: National Cancer Data Base. Cancer. 2016;122:1523-1532.
- Hosmer DW, Lemeshow S, Sturdivant RX. Applied Logistic Regression. John Wiley and Sons, Inc. 2013.
- Ang KK, Harris J, Wheeler R, et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N Eng J Med. 2010;363:24-35.
- Nichols AC, Theurer J, Prisman E, et al. Radiotherapy versus trans-oral robotic surgery and neck dissection or oropharyngeal squamous cell carcinoma (ORATOR): an open label, phase 2, randomized trial. Lancet Oncol. 2019;20(10)1349-1359. doi: https://doi.org/10.1016/S1470-2045(19)30410-3
- Mahmoud O, Sung, K, Civantos FJ, et al Transoral robotic surgery for oropharyngeal squamous cell carcinoma in the era of human papillomavirus. Head Neck. 2018;40:710-721.
- Yokota T, Iida Y, Kamijo T, et al. Which treatment strategies are the most promising for locally advanced resectable human papillomavirus-associated oropharyngeal cancers? J Clin Oncol. 2019;37:15_suppl. doi:10.1200/JCO.2019.37.15_suppl.e17556
- Van Abel KM, Quick MH, Graner DE, et al. Outcomes following TORS for HPV-positive oropharyngeal carcinoma: PEGs, tracheostomies, and beyond. Am J Otolaryngol. 2019;40(5)729-734. doi 10.1016/j.amjoto.2019.07.003
- Roden DF, Hobelmann K, Vimawala S, et al. Evaluating the impact of smoking on disease-specific survival outcomes in patients with human-papillomavirus-associated oropharyngeal cancer treated with transoral robotic surgery. Cancer. 2020:126;9. doi:10.1002/cncr.32739
- Dhanireddy B, Burnett NP, Sanampudi S, et al. Outcomes in surgically resectable oropharynx cancer treated with transoral robotic surgery versus definitive chemoradiation. Am J Otolaryng. 2019;40(5);673-677. doi: 10.1016/j.amjoto.2019.06.001
- Ferris RL, Flamand Y, Weinstein GS, et al. Transoral robotic surgical resection followed by randomization to low- or standard dose IMRT in resectable p16+ locally advanced oropharynx cancer: a trial of the ECOG-ACRIN Cancer Research Group (E3311). J Clin Onc. 2020;38:suppl; abstr 6500. doi: 10.1200/JCO. 2020. 38.15_suppl.6500
- Yom SS, Torres-Saavedra P, Caudell JJ, et al. NRG-HN002: A randomized phase ii trial for patients with p16-positive, non-smoking-associated, locoregionally advanced oropharyngeal cancer. IJROBP 2020;105(3);684-685.
- Gillison ML, Trotti, AM, Harris J, et al. Radiation therapy plus cetuximab or cisplatin in human papillomavirus-positive oropharyngeal cancer (NRG Oncology RTOG 1016): a randomized, multicenter, non-inferiority trial. Lancet 2019;393(10166):40-50. doi:10.1016/S0140-6736(18)32779-X
Citation
AM T, KN M, JA G, S L, G S, Y H, V A. Upfront Surgery With Adjuvant RT Vs Chemoradiation in HPV-Mediated Oropharyngeal Cancer in Intermediate-Risk Patients. Appl Radiat Oncol. 2021;(1):28-35.
March 30, 2021