Use of an OP Care smartphone application to improve care of gynecology cancer patients in a low-resource setting
Images
With 10 million new cancer diagnoses expected annually by 2030, low- and middle-income countries (LMICs) are expected to see an increase of cancer incidence.1 Currently, > 60% of the global cancer burden and 70% of cancer-related mortality occur in LMICs.2 In these regions, there is a need for access to early detection, affordable treatment, and integrated treatment monitoring. This case summary describes the use of a smartphone application to monitor treatment initiation and follow-up of patients with gynecologic cancers who presented to the multidisciplinary team clinic (MDT) at Princess Marina Hospital, Gaborone, Botswana.
CASE SUMMARY
Following the success of 2 digital health pilot studies in LMICs3,4 in January 2018, the clinic adopted OP Care, an outpatient smartphone application developed by ONE BCG Pty Ltd (Gaborone, Botswana, Africa). OP Care is able to: 1) store and share patient oncology records with restricted access to users, 2) electronically schedule appointments including automatic reminders to patients and notifications of missed appointments to providers, and 3) display real-time clinic reports. OP Care provides a user-friendly interface that enables physicians, nurses, and students to enter information into an electronic form and add notes and attachments. The average time to enter patient data into the application is lower than previously used paper records. The application’s electronic link to Google Data Studio enables real-time deidentified reports of parameters including age, gender, HIV status, cancer type, cancer stage, treatment intent, treatment type, appointments completed, appointments missed, and short message services (SMS) sent.
From January 2018 to March 2019, OP Care was used to enroll 751 patients, of whom 506 (67.4%) were enrolled from the gynecologic MDT clinic and 245 (32.6%) were from the general oncology unit. Of all enrolled patients, 401 (53.4%) were aged 40 to 60 years, 647 (86.2%) were female, 376 (50.1%) were HIV-positive, and 437 (58.2%) were treated with curative intent therapy. Addionally, 432 (71.6%) patients were diagnosed with cervical cancer, 263 (35.0%) were stage II/III, and 61 (10.1%) had an unknown stage.
In total, OP Care tracked 1103 completed appointments and 415 missed appointments. Missed appointments are stratified by appointment type: 102 (24.6%) were follow-ups after treatment, 159 (38.3%) were for treatment review, 138 (33.3%) were generic appointments, and 3 (0.72%) were for offsite treatment. Unfortunately, missed appointments were not recorded in the resister for use in evaluating the compliance rate prior to OP care. During the period, 2492 short message services (SMS) were sent to remind patients of their appointments, of which 2,370 (95.1%) were successfully received by the patient on a feature phone. Of the 751 cases, < 5 patients had no cell phone of any kind and had messages sent to their care provider (eg, son, daughter).
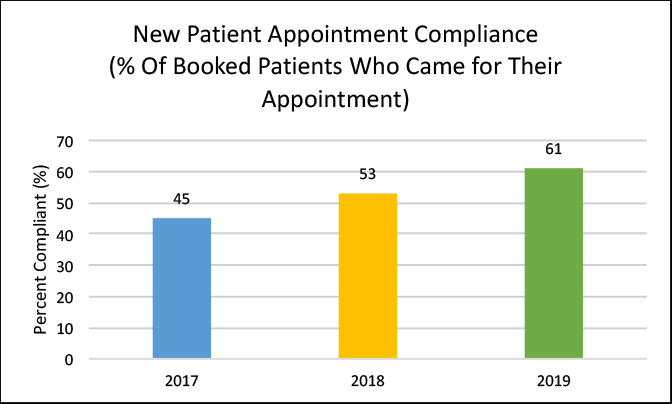
We reviewed new patient booking data in the MDT clinic from 2017-2019 to assess whether the patient attendance rate improved with implementation of OP Care. In 2017 (May to December), before implementation of OP Care, an average of 45% of the patients :(based on a total of 561 patients) booked for clinic actually came (prior to that, data was not available since the registers were not saved). In Feburary 2018, OP Care was initiated in the clinic, with very few patients (< 1%) declining consent to enroll. In 2018, the attendance rate improved to 53%. The attendance rate for 2019, with OP Care fully implemented, from January to June, was 61%. Thus, between 2017 to 2019 (before and after OP Care initiation) there was a 33% increase in patients arriving to booked appointments, which was statistically significant using a t-test (p = 0.02) (Figure 1).
DISCUSSION
Through Botswana’s national insurance system, citizens usually have access to all treatment modalities required based on cancer stage at full cost to the government. However, similar to other LMICs, oncology care in Botswana suffers from a high patient burden accompanied by a lack of personnel and lack of robust referral and follow-up systems.5
The gynecologic oncology MDT clinic integrates patient care into a single setting by assessing new and follow-up patients. All new patients are examined by oncology and gynecology physicians, and departments agree on a patient treatment plan. The clinic facilitates early review of new cancer cases by all necessary departments in the hospital as well as private facilities with the intention to educate patients about their diagnosis and treatment plan, decrease treatment delays as well as facilitate access to palliative care and social work interventions. Treatment and patient outcomes are reported during follow-up, which is crucial to identify disease recurrence/progression and establish appropriate patient management. The objective of post-treatment follow-up is to educate patients on late treatment side effects and how to manage them, and refer the patients if necessary to other specialists for intervention.6,7 Since its conception in May 2015, the MDT clinic has seen over 1000 patients. However, during this period, in addition to poor physician-to-patient ratios,8 challenges included incomplete hospital inventory of paper-based medical records,5,9 fragmented communication between physicians and social work,5 and patient loss to follow-up.10 The barriers in structured communication resulted in no treatment initiation, delays in treatment, and/or inconsistent follow-up.5-10
A cross-sectional study surveying providers who used the application and patients enrolled via the application was conducted to assess the usability and effectiveness of OP Care.11 The study found that 78% of providers did not feel OP Care increased their work burden and they were willing to use the application.11 In addition, based on 19 questions regarding usability, providers stated they were very comfortable using OP Care.11 Patients felt SMS reminders were very helpful, but preferred messages in Setswana instead of in English.11 Further, attendance of scheduled new patient appointments has increased from 45% to 60% in just over a year since implementing OP Care and patient reminders. We will continue to follow OP Care data for new patients and follow up on patients over time as the OP Care application continues to be modified to further improve patient follow-up and retention rates. In the long term, we also plan to study reduction in patient delays and improvement in patient outcomes as a result of OP Care implementation. Thus far, we believe the integration of OP Care into the clinic has improved access to medical records, clinic schedules, and patient follow-up, allowing the healthcare workers to focus on patient management and treatment counseling. The healthcare team can spend more time on patient care instead of worrying about obtaining medical records and managing the schedule.11
Despite the SMS reminders, several appointments were missed. Although there are no data from the MDT clinic on reasons for missed appointments, a recent study in Botswana evaluated reasons for missed appointments. In a cohort of 488 patients, 172 missed appointments due to work obligation, family duties, transportation fees, and forgetting the appointment date.12 While OP Care will not be able to improve missed appointments due to work and family obligations, we hypothesize that SMS reminders will decrease missed appointments from forgotten appointment dates. In addition, due to poor death registration, some patients lost to treatment may have died. OP Care will add questions for reason of missed appointments to help develop problem-specific interventions.
CONCLUSION
The use of OP Care in a LMIC gynecology oncology clinic setting demonstrates the feasibility and efficacy of user-friendly mobile technology to improve patient record storage, treatment monitoring, appointment scheduling and tracking as well as patient compliance with booked appointments. In addition, real-time data output enables personnel of varying skill to assess clinic data, providing a simple method for clinics to identify gaps and measure quality improvement. We plan to expand use of this application to other oncology clinics as well as other specialties. Future steps also include studying improvement in patient retention and outcomes as a result of an OP Care application.
REFERENCES
- World Health Organization. Cancer. Key Statistics. https://www.who.int/cancer/resources/keyfacts/en/. Accessed October 17, 2019.
- Moten A, Schafer D, Ferrari M. Redefining global health priorities: improving cancer care in developing settings. J Glob Health. 2014;4(1).
- Stephan LS, Almeida ED, Guimarães RB, et al. Oral anticoagulation in atrial fibrillation: development and evaluation of a mobile health application to support shared decision-making. Arq Bras Cardiol. 2018;110(1):7-15.
- Coppock D, Zambo D, Moyo D, et al. Development and usability of a smartphone application for tracking antiretroviral medication refill data for human immunodeficiency virus. Methods Inf Med. 2017;56(05):351-359.
- Fundytus A, Sullivan R, Vanderpuye V, et al. Delivery of global cancer care: an international study of medical oncology workload. J Glob Health. 2017;4:1-11.
- Grover S, Raesima M, Bvochora-Nsingo M, et al. Cervical cancer in Botswana: current state and future steps for screening and treatment programs. Front Oncol. 2015;5:239.
- Grover S, Chiyapo SP, Puri P, et al. Multidisciplinary gynecologic oncology clinic in Botswana: a model for multidisciplinary oncology care in low-and middle-income settings. J Glob Health. 2017;3(5):666-670.
- LaVigne AW, Triedman SA, Randall TC, Trimble EL, Viswanathan AN. Cervical cancer in low and middle income countries: addressing barriers to radiotherapy delivery. Gynecol Oncol Rep. 2017;22:16-20.
- Randall TC, Ghebre R. Challenges in prevention and care delivery for women with cervical cancer in sub-Saharan Africa. Front Oncol. 2016;6:160.
- Dickinson R, Hall S, Sinclair JE, Bond C, Murchie P. Using technology to deliver cancer follow-up: a systematic review. BMC Cancer. 2014; 14(1):311.
- Shah S, Monare B, Urusaro S, et al. Usability and effectiveness of smartphone application for tracking oncology patients in Gaborone, Botswana. Abstract presented at: Consortium of Universities for Global Health; March 8-10, 2019; Chicago, IL.
- Tapela N, Gabegwe K, Barak T, et al. Barriers to cancer evaluation follow-up: Reasons and predictors of missed visits in a rural population in Botswana. J Glob Health. Abstract; 2018.
Citation
TB R, S D, N B, B M, G D, S G. Use of an OP Care smartphone application to improve care of gynecology cancer patients in a low-resource setting. Appl Radiat Oncol. 2019;(4):38-40.
December 28, 2019