Future of Radiation Oncology Education: Transforming Scholarly Teaching Into Medical Education Scholarship
Images

SA-CME credits are available for this article here.
Abstract
Medical education is vital in preparing radiation oncologists to care for patients in an ever-changing landscape of new treatments and technologies. Medical education must develop and adapt through robust education scholarship, utilizing novel teaching with evidence-based best practices to optimally teach new concepts. Education scholarship has led to significant advances in several areas of radiation oncology education, spanning undergraduate medical education (UME); graduate medical education (GME); continuing medical education (CME); and diversity, equity, and inclusion (DEI). Continued growth in these domains are critical for the future of our field, and education scholarship can facilitate these advances.
Due to technical advances and changing treatment paradigms, the knowledge required to practice radiation oncology continues to evolve, necessitating a comprehensive and ever-changing set of educational tools to train a spectrum of learners. Over the past two decades, academic medicine, and specifically the field of radiation oncology, has seen an increasing focus on medical education.1 This is likely multifactorial and attributable in part to an increase in learner’s needs, such as the need for high-yield teaching due to time limitations in educational settings, desire for more flexible learning options, and a generally higher standard of education exposure/expectations from a systemically more mature educational community. Increasing attention to vulnerable populations and the importance of diversity, equity, and, inclusion (DEI) in health care and medical training has also fueled educational interventions and innovations.2-4 In response to this increasing focus on the value of medical education, many US institutions now consider medical education scholarship when evaluating academic faculty for promotion.5 Here we describe differences between scholarly teaching and the scholarship of teaching before focusing on impactful areas of current and future medical education scholarship within radiation oncology, with a focus on undergraduate medical education (UME); graduate medical education (GME); and continuing medical education (CME); and diversity, equity, and inclusion (DEI). With educational innovation and educational scholarship, the future of radiation oncology education is bright.
Defining Medical Education Scholarship
Dissemination of medical education scholarship is needed to synergize efforts across institutions, and to create a foundation upon which future efforts can further advance education. In this discussion, it is important to differentiate teaching methods within medical education (an umbrella term encompassing multiple practices in teaching hospitals) between those that specifically draw on best practices and evidence-based methods, here referred to as scholarly teaching, from nonevidence-based teaching methods. Scholarly teaching is similarly distinct from, though may overlap with, education scholarship, the process of moving the field of medical education forward by rigorously measuring, assessing, and reporting on the results of scholarly teaching for publication.6 These distinctions are important because the advancement of medical education relies on both the development of scholarly teaching methods and the robust assessment and dissemination of the results of these interventions. To ensure that scholarly efforts in medical education qualify as rigorous education scholarship, scholars may look to Glassick’s 6 standards for educational scholarship: 1) clear goals, 2) adequate preparation, 3) appropriate methods, 4) significant results, 5) effective presentation, and 6) reflective critique.7 While interventional studies and prospective trials are a
common form of clinical research, impactful educational scholarship can focus on innovative teaching methods, novel educational materials, qualitative survey and focus group assessment, and curriculum design, among other examples.
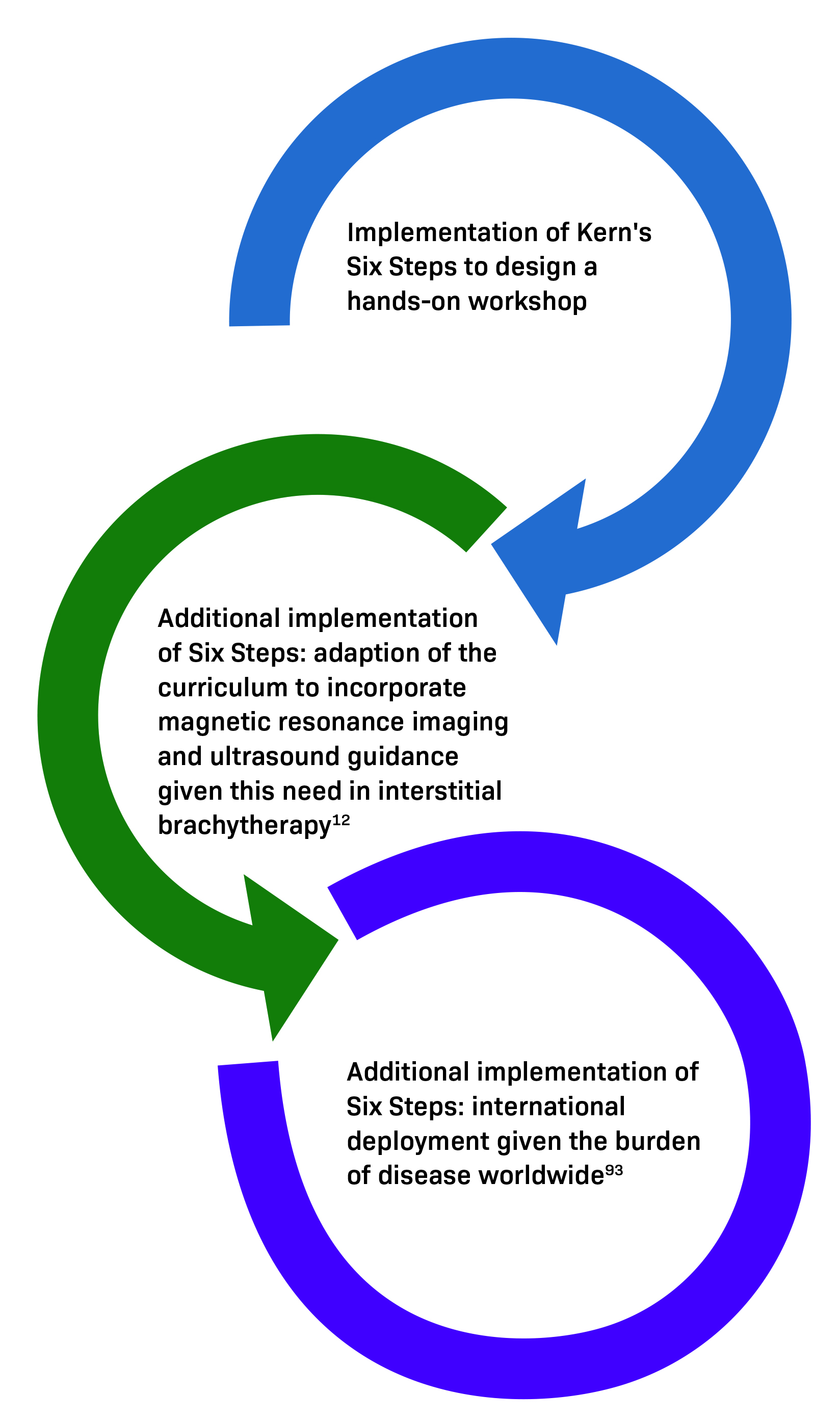
One of the most common types of medical education scholarship in radiation oncology is curriculum development,8-10 for which an established framework is Kern’s Six Steps (Figure 1A).11 These steps help ensure that Glassick’s criteria are met using a structured approach to curriculum development. For example, Figure 1A illustrates a needs assessment of a simulation-based educational workshop for GME and CME learners.12,13 Evaluation of this workshop led to curriculum adjustments and additional implementations of Kern’s Six Step Approach (Figure 1B),14 which is cyclical and can be used for continuous educational innovation. Overall, it is important to be methodical and intentional to transform scholarly activity to scholarship.
Undergraduate Medical Education
In the UME setting, medical education can be used to increase exposure to radiation oncology, which is critical for maintaining a workforce as well as preparing those in other specialties to understand when to consult radiation oncology. For students rotating in radiation oncology, an evidence-based national UME curriculum in radiation oncology is also critical given that the field is rapidly evolving, with new technology and management indications growing from year to year. It is documented that UME rarely incorporates information about radiation oncology, while exposure increases medical student interest and affinity for the specialty.9,15,16
In UME, most school curricula do not include a dedicated radiation oncology didactic session in their preclinical curricula17 and some students may not gain exposure to any aspect of radiation oncology throughout their medical school education.9,18,19 Novel methods of incorporating radiation oncology into the medical school curriculum can include collaborating with preclinical course leaders or integrating radiation oncology into a clinical rotation.20,21 Radiation oncology can also be incorporated into a general oncology educational curriculum. One example of this is the Scholars in Oncology-Associated Research (SOAR) cancer research education program, a summer research experience for first-year medical students at the University of Chicago, which includes a formalized interdisciplinary and interprofessional oncology curriculum, such as 10 2-hour lectures, tumor board attendance, and half-day shadowing with a pharmacist, therapist, or palliative care advanced practice nurse.22 This program has demonstrated that preclinical students had an increased understanding of the multidisciplinary nature of oncology, including radiation oncology, after completion of the program.
In the preclinical setting, a single lecture on radiation oncology has been shown to significantly increase medical student knowledge of the field, as well as increase desire to learn more about the field.23,24 In the clinical setting, the introduction of an optional radiation oncology rotation during a core surgery clerkship for third-year medical students was shown to significantly improve radiation oncology knowledge and usefulness of the knowledge in their careers.20 Furthermore, a structured didactic curriculum in radiation oncology significantly improved knowledge and clinical competency, suggesting that structured didactics are important to a well-designed clerkship.25-27
In addition to novel educational programs in medical school, mentorship initiatives can also promote student interest and engagement in the field of radiation oncology. A large, formalized mentorship program described by Hirsch et al, with both clinical and research tracks, demonstrated that mentorship significantly impacts specialty selection and productivity in the field.28,29 This mentorship initiative was associated with high mentee satisfaction and improved confidence in the residency application process.30 Similar results have been reported from other mentorship pilot programs in recent years.31,32
In the COVID era, there has been a new emphasis on creating virtual mentorship and educational opportunities, which allows for expanded access to the field, even for those who attend a school without an associated radiation oncology residency program. The Radiation Oncology Virtual Education Rotation (ROVER) is one example of a novel virtual experience that implemented educational panels and case-based learning, which significantly improved medical student understanding of the role of radiation oncology in a number of disease sites.33 Other published experiences with virtual clinic, tumor boards, and didactics in the medical student population have yielded similar results with high satisfaction rates.34 The Radiation Oncology Intensive Shadowing Experience (RISE), a virtual educational and mentorship initiative for under-represented medical students, was recently implemented to help reduce the disparities in access and exposure to radiation oncology during the COVID-19 pandemic; this added to the literature questions on optimal implementation of scholarly teaching for URM students in a virtual environment, as well as reported on experiences of both mentees and mentors in this understudied educational environment.35 Of the 14 URM students participating in RISE, 100% completed pre- and post-surveys with the majority agreeing strongly that they planned to utilize what they learned for their future practice (93%). This unique program centering equity and inclusion within medical education was not only feasible but desired and highly rated by participants.36 The above initiatives differ in size and scope, but all provide pathways to drive medical student interest in the field. Future directions should focus on optimizing the design, development, implementation, evaluation, and ongoing sustainability of these educational and mentorship programs as an integral part in the formation of the next generation of radiation oncologists.
Graduate Medical Education
The national requirements for radiation oncology residency training involve Accreditation Council for Graduate Medical Education (ACGME) case log requirements, American Board of Radiology (ABR) written and oral certification exams, and American College of Radiology (ACR) in-training written exams. However, the overall curriculum is left to individual residency and fellowship training programs. To provide guidance to US training programs with regard to GME curriculum, the Radiation Oncology Education Collaborative Study Group (ROECSG) formed a Core Curriculum Leadership Committee utilizing the Delphi method to identify and develop content domains (CDs) and entrustable professional activities (EPAs) to formalize a curricular framework for radiation oncology GME in the United States.37 A strength of this process is the inclusion of numerous radiation oncology GME stakeholders, including academic and private practice physicians, residents, physicists, dosimetrists, nurses, therapists, and others to ensure a well-balanced curriculum.
Novel educational initiatives that leverage technology to facilitate learning in residency also have the potential to improve medi- cal education. Recent work on web-based educational tools for residents focusing on anatomy and contouring guidelines has improved resident confidence and competence in these areas.38,39 A case bank learning tool on radiation treatment plan evaluation from Princess Margaret Cancer Centre has also been shown to improve resident competency, with a pilot study demonstrating that a high-fidelity simulation platform was associated with increased learning and competency attainment.40 A common limitation in these studies utilizing web-based or technology-oriented teaching is the reproduction of these tools outside of the institution, whether due to intellectual property concerns or resource concerns (ie, when an institution may not have the same software available to their learners). Another concern was the need for continuous information technology upkeep and maintenance that may require funding and resources. Finally, specialty curricula in radiation oncology residency have been developed in several niche areas such as global oncology41 and quality and safety,42 among others, with the intent that more robust education will increase career interest and progress in areas of critical need. With the increasing field complexity and growing knowledge required to be a radiation oncologist, work on innovative learning tools should be prioritized.
Future GME efforts can also focus on transition to practice. Although residency is ultimately intended to prepare physicians for independent practice, the transition from resident to attending physician is often challenging, especially in areas of limited exposure during training. Within radiation oncology, multiple surveys, editorials, and focus groups have described the encountered or anticipated obstacles involved in adjusting to unsupervised clinical care during transition to independent practice.43-47 Commonly cited issues include inadequate exposure to certain clinical competencies, such as treatment plan review and image verification, and limited guidance about nonclinical responsibilities, including leadership,48,49 mentorship,31 and education.50 Currently, there are few widely available resources to develop proficiencies in plan review51,52 or image verification, while resources provided by individual programs can vary significantly, or more often are lacking altogether.53 Scholarship of simulation-based teaching has shown substantial impact in acquisition of practical skills and, to date in radiation oncology, simulation-based teaching has been created for plan review40 and image verification,54 although it has broad applicability for other radiation oncology skills, including treatment planning and toxicity management. As part of a collective effort through ROECSG, a series of workshops to structure the teaching of the basic components of plan evaluation – called the Radiation Oncology Plan Evaluation School (ROPES) – is in progress.55 This project draws on expert consensus from multiple institutions to develop a practical educational tool to evaluate several acceptable plans in the same patient scenario. Likewise, select programs are aimed at enhancing leadership56-58 and teaching59 skills to utilize best practices in individual environments. Another ongoing ROECSG effort is the Teaching Mentoring in Radiation Oncology (TEAMRO) program designed to develop mentoring talents among residents,60 with a multi-institutional pilot program underway investigating whether formalized mentoring of students by residents can impact a resident’s mentorship relations and education overall.
In addition to individual interventions targeting specific deficiencies, another approach would be to augment resident autonomy overall. For example, continuity clinics and “transition-to-practice” services are experiences designed to position residents as the primary care provider with appropriate supervision. While these are common across the medical field,61-64 few programs in radiation oncology have been described. Of the published experiences, the most comprehensive resident-led rotations include the senior resident rotation at Mayo Clinic65 and the Veterans Affairs Medical Center rotation in Duke’s radiation oncology residency training program;66 however; there is a need for more robust and longitudinal scholarship demonstrating beneficial translation of these experiences into clinical practice. Both programs facilitate autonomy by allowing the resident to assume responsibility for most patient care tasks, including clinical encounters, management recommendations, documentation, directing radiation therapy planning and delivery (ie, simulation, contouring, plan evaluation, image verification), and interdisciplinary communication and collaboration. While there is attending oversight, the attending assumes a consultant role for the trainee, allowing the resident greater independence and responsibility, mimicking independent practice. Another option to promote autonomy is a continuity clinic for follow-up visits, as at the University of Southern California.67 These clinics have been reported to improve resident confidence while addressing core issues during early independent practice.67 Widespread use of resident-led follow-up clinics may be limited because of institutional and ACGME supervision policies but warrant additional consideration.
Continuing Medical Education
With the continuing technical advances and evidence-based clinical practice shifts in radiation oncology, the need for education does not end after residency training. With practice-changing clinical trials in radiation oncology, medical oncology, and surgery, the standard of care in any disease site continues to evolve. Although states differ in the number and type of CME credits required (for exam- ple AMA category 1, vs AMA category 2, vs self-assessment or SA-CME), CME credits are required for state licensing, American Board of Radiology (ABR) certification and maintenance of certification (MOC). AMA Category 2 credit is self-designated, allowing physicians to claim credit for educational activities such as peer review, provided the activity meets AMA standards. Radiation oncologists may already engage in these activities at their practices. Self-assessment CME (SA-CME) is a subtype of CME that includes content followed by related questions. SA-CME has been historically required for physicians to maintain certification with ABR. Recently, the ABR announced that participation in MOC and online longitudinal assessment (OLA) would fulfill the SA-CME requirement, removing the need to complete additional self-assessment modules to meet ABR requirements.68 It is unknown if this change will impact quality or utility of CME. Outside of self-assessment, CME enables radiation oncologists to stay current on treatments, planning techniques, and toxicity management. Annual meetings for radiation oncology professional societies provide CME opportunities. In addition, many institutions offer oncology-specific CME courses. Virtual access to these meetings during the COVID-19 pandemic enabled learning without travel, and continued virtual opportunities may improve future CME access.
Educational needs for practicing radiation oncologists also may be driven by changes in practice throughout a career, such as treating new disease sites, or by a practice acquiring new technology. Web-based contouring tools such as eContour provide a resource for ongoing contouring education for radiation oncologists across the world.69,70 On-the-job mentorship in brachytherapy was encouraged through the American Brachytherapy Society #NextGenBrachy initiative.71 Novel simulation-based workshops in brachytherapy have also been beneficial, and simulation-based education may enhance CME in other areas in the future.12,72 Currently, the ACR offers a number of multiday hands-on educational experiences for practicing radiologists focusing on topics such as breast MRI and nuclear medicine. In the future, similar courses for radiation oncologists could facilitate practice transitions or vendor-neutral understanding of new technology in a practice.
Technological advances in radiation oncology will also drive new CME needs, such as with online adaptive planning for external-beam radiation therapy. Both CT- and MR-based systems are now widely available for commercial use, necessitating the development of new physician workflows and education for clinicians unfamiliar with this technology.73,74 Future work in the medical education space should also focus on artificial intelligence (AI) in clinical practice, such as AI-based contouring and treatment planning.75
As multiple recent studies have demonstrated, auto segmentation with AI and machine learning models can delineate some target volumes and organs at risk while significantly improving efficiency across disease sites.76-80 Multiple recent studies have also shown a potential role for AI-based treatment planning and optimization.81-83 Better understanding of AI could also facilitate radiation oncology research in optimizing clinical workflow, prognosticating patient and personalization of management decisions, and identifying patients at risk of toxicity who require greater clinical attention, among other areas. Finally, AI-based tools may also be introduced into medical education to optimize teaching the next generation of learners.84 One example is a study that found deep-learning models could take full videos of surgeons performing surgical techniques for assessment, categorize them into individual surgical steps, and assess performance levels, suggesting a framework for assessing technical skills that may be difficult to quantify with examinations.85 CME scholarship in adaptive radiation therapy, AI, and other areas of growth will facilitate future medical education needs for radiation oncologists in practice.
Advancement of Diversity, Equity, and Inclusion
Integration of diversity, equity and inclusion (DEI) principles and practices throughout all aspects of medical education (UME, GME, and CME) are critical to workforce training. Ultimately, the creation of clinically applicable and sustainable education solutions that ad- vance diversity require strategies that involve all aspects of medical education and include not only underrepresented-in-medicine (UIM) physicians, but also non-UIM physicians, patients, and hospital systems.
In radiation oncology, a virtual away rotation is a medical education initiative that addresses DEI issues in clinical learning environments.86,87 RISE is one such example of intentionally targeting opportunities to learn about radiation oncology and UIM medical students.35 The RISE program demonstrates an example of transforming education research in DEI from scholarly teaching to scholarship, as authors utilize pre- and post-surveys to investigate how scholarly teaching impacted both teachers and learners in a novel environment, with results serving to improve future iterations of scholarly teaching in the virtual environment. There are also in-person opportunities, such as in the Department of Radiation Oncology at the Washington University School of Medicine in St. Louis, which offers a 1-month medical student rotation for fourth-year medical students from diverse backgrounds through the Diversity & Inclusion Clerkship Opportunity for Underrepresented Medical Students (D.I.C.O.M.S.) program. The rotation includes a $2000 stipend to help offset the cost of travel, housing, Visiting Student Application Service (VSAS), and incidental expenses. National radiation oncology organizations, such as the American Society for Radiation Oncology (ASTRO), also have dedicated opportunities for medical students and early career faculty from underrepresented groups. Two examples are the ASTRO Minority Summer Fellowship Award, which exposes medical students to clinical, basic and translational research questions in radiation oncology, and the ASTRO Leadership Pipeline Program (formerly known as the Pipeline Protégé Program), a career development program aimed at increasing diversity among ASTRO leadership. Overall, as examples of scholarly teaching in DEI for radiation oncology grow, so does the need for medical education scholarship of such initiatives, highlighting the importance of evaluating and reporting on the impact of scholarly teaching on URM students, and radiation oncology trainees and practitioners, to inform and advance the field for our colleagues, patients, communities, and ourselves.
Radiation oncology residents have also addressed the need for DEI training by establishing the Subcommittee on Equity and Inclusion as part of the Association of Residents in Radiation Oncology (ARRO). The goal of the subcommittee is to foster a supportive environment for trainees, systematically assessing and reporting trends in workforce diversity, and initiating and fostering ongoing dialogue on issues of DEI and social justice.88 With studies demonstrating ongoing workforce disparities89 and the subsequent impact on health equity,90 it is critical that we move toward implementation and assessment of these and other DEI-centered interventions91 to foster sustainability and reproducibility across specialties.92
Conclusion
Radiation oncology medical education is at an important inflection point where a heightened interest in educational innovation is meeting increased needs for research and innovation in critical topics across UME, GME, CME, and DEI. This article has noted several examples of education scholarship that have increased opportunity for further research into critical areas. Scholarship on mentorship with medical students has improved mentorship practices in other areas of radiation oncology. Curriculum design on special topics such as simulation-based education in brachytherapy at the GME level has led to robust curriculum design of other special topics of critical need in early training and education of other technological advances, including simulation-based training in online adaptive radiation therapy at the CME level. Results in pilot studies investigating educational approaches for UIM students suggest that DEI education can improve training and patient care. Continued efforts in education and educational scholarship can advance best practices and evidence-based approaches for teaching, both of which are essential to train a diverse future workforce in evidence-based cancer treatment.
References
- Rosenberg DM, Braunstein SE, Fields EC, et al. Radiation oncology education collaborative study group annual spring symposium: initial impact and feedback. J Cancer Educ. Published online March 16, 2021. doi:10.1007/s13187-021-01990-8
- Daniel M, Gordon M, Patricio M, et al. An update on developments in medical education in response to the COVID-19 pandemic: A BEME scoping review: BEME Guide No. 64. Med Teach. 2021;43(3):253-271. doi:10.1080/0142159X.2020.1864310
- Eva KW. Publishing during COVID-19: Lessons for health professions education research. Med Educ. 2021;55(3):278-280. doi:10.1111/medu.14450
- Fernandez A. Further incorporating diversity, equity, and inclusion into medical education research. Acad Med. 2019;94(11S):S5. doi:10.1097/ ACM.0000000000002916
- Lubitz RM. Guidelines for promotion of clinician-educators. J Gen Intern Med. 1997;12(Suppl 2):S71-S78. doi:10.1046/j.1525-1497.12.s2.10.x
- Fincher RM, Simpson DE, Mennin SP, et al. Scholarship in teaching: an imperative for the 21st century. Acad Med. 2000;75(9):887-894. doi:10.1097/0000188 8-200009000-00009
- Glassick CE. Boyer’s expanded definitions of scholarship, the standards for assessing scholarship, and the elusiveness of the scholarship of teaching. Acad Med. 2000;75(9):877-880. doi:10.1097/00001888-200009000-00007
- Christensen MT, Kumar KA, Wang WS, Dharmarajan KV, Siropaides CH. Development of patient-centered communication curriculum for radiation oncology residents. Int J Radiat Oncol Biol Phys. 2022;114(1):e12. doi:10.1016/j.ijrobp.2022.06.021
- Oskvarek J, Braunstein S, Farnan J, et al. Medical student knowledge of oncology and related disciplines: a targeted needs assessment. J Cancer Educ. 2016;31(3):529-532. doi:10.1007/s13187-015-0876-2
- Buckley L, Bacha B, Gaudet M, et al. Development of a curriculum for the implementation of stereotactic radiation therapy programs in middle-income countries. JCO Glob Oncol. 2022;8:e2100389. doi:10.1200/GO.21.00389
- Thomas PA, Kern DE, Hughes MT, Chen BY. Curriculum Development for Medical Education: A Six-Step Approach. J. Hopkins Uni. Press; 2015. Accessed September 29, 2022. https://jhu.pure.elsevier.com/en/publications/curriculum-development-for-medical-education-a-six-step-approach
- Singer L, Braunstein S, Klopp A, Joyner M. Development and implementation of a simulation-based educational workshop on gynecological brachytherapy: pilot study at a national meeting. Pract Radiat Oncol. 2019;9(5):e465-e472. doi:10.1016/j.prro.2019.05.006
- Gaudet M, Jaswal J, Keyes M. Current state of brachytherapy teaching in Canada: a national survey of radiation oncologists, residents, and fellows. Brachytherapy. 2015;14(2):197-201. doi:10.1016/j.brachy.2014.11.004
- Fields EC, Joyner MM, Singer L, Todor D. A new development in ultrasound-compatible gynecologic brachytherapy simulators. Brachytherapy. 2020;19(6):783-786. doi:10.1016/j.brachy.2020.09.011
- Mattes MD, Patel KR, Burt LM, Hirsch AE. A nationwide medical student assessment of oncology education. J Cancer Educ. 2016;31(4):679-686. doi:10.1007/ s13187-015-0872-6
- Agarwal A, Shah A, Shah B, Koottappillil B, Hirsch AE. The impact of a radiation oncologist led oncology curriculum on medical student knowledge. J Cancer Educ. 2018;33(6):1176-1180. doi:10.1007/s13187-017-1227-2
- Zaorsky NG, Shaikh T, Handorf E, et al. What are medical students in the United States learning about radiation oncology? Results of a multi-institutional survey. Int J Radiat Oncol Biol Phys. 2016;94(2):235-242. doi:10.1016/j.ijrobp.2015.10.008
- Arbab M, Holmes JA, Olivier KR, et al. Integrating radiation oncology into undergraduate medical education. Adv Radiat Oncol. 2021;6(6):100765. doi:10.1016/j. adro.2021.100765
- Mattes MD, Deville C, Vega RBM, et al. Demographics of ASTRO student members and potential implications for future U.S. radiation oncology workforce diversity. Adv Radiat Oncol. 2022;7(2):100834. doi:10.1016/j.adro.2021.100834
- Zaorsky NG, Malatesta TM, Den RB, et al. Assessing the value of an optional radiation oncology clinical rotation during the core clerkships in medical school. Int J Radiat Oncol Biol Phys. 2012;83(4):e465-e469. doi:10.1016/j.ijrobp.2012.01.058
- Zaorsky NG, Malatesta TM, Showalter TN, et al. Impact of a radiation oncology elective on the careers of young physicians: update on a prospective cohort study.Int J Radiat Oncol Biol Phys. 2013;86(2):214-215. doi:10.1016/j.ijrobp.2013.02.001
- McKillip RP, Hahn OM, Bartkowiak B, et al. Implementation of a novel medical school multidisciplinary and interprofessional oncology curriculum: a mixed method study. J Cancer Educ. 2019;34(1):50-55. doi:10.1007/s13187-017-1264-x
- Hirsch AE, Bishop PM, Dad L, Singh D, Slanetz PJ. An increase in medical student knowledge of radiation oncology: a pre–post examination analysis of the oncology education initiative. Int J Radiat Oncol Biol Phys. 2009;73(4):1003-1008.e2. doi:10.1016/j.ijrobp.2008.12.012
- Hirsch AE, Handal R, Daniels J, et al. Quantitatively and qualitatively augmenting medical student knowledge of oncology and radiation oncology: an update on the impact of the oncology education initiative. J Am Coll Radiol. 2012;9(2):115-120. doi:10.1016/j.jacr.2011.07.001
- Golden DW, Kauffmann GE, McKillip RP, et al. Objective evaluation of a didactic curriculum for the radiation oncology medical student clerkship. Int J Radiat Oncol Biol Phys. 2018;101(5):1039-1045. doi:10.1016/j.ijrobp.2018.04.052
- Golden DW, Spektor A, Rudra S, et al. Radiation oncology medical student clerkship: implementation and evaluation of a bi-institutional pilot curriculum. Int J Radiat Oncol Biol Phys. 2014;88(1):45-50. doi:10.1016/j.ijrobp.2013.10.041
- Jagadeesan VS, Raleigh DR, Koshy M, Howard AR, Chmura SJ, Golden DW. A national radiation oncology medical student clerkship survey: didactic curricular components increase confidence in clinical competency. Int J Radiat Oncol Biol Phys. 2014;88(1):51-56. doi:10.1016/j.ijrobp.2013.11.206
- Hirsch AE, Agarwal A, Rand AE, et al. Medical student mentorship in radiation oncology at a single academic institution: a 10-year analysis. Pract Radiat Oncol. 2015;5(3):e163-e168. doi:10.1016/j.prro.2014.08.005
- Huang D, Qureshi MM, Sarfaty S, et al. Longitudinal outcomes of medical student research mentorship: a 15-Year analysis of the radiation oncology mentorship initiative. J Cancer Educ. Published online September 24, 2021. doi:10.1007/s13187-021-02091-2
- Boyd GH, Rand AE, DeNunzio NJ, Agarwal A, Hirsch AE. The radiation oncology mentorship initiative: analysis of a formal mentoring initiative for medical students interested in radiation oncology. J Cancer Educ. 2020;35(5):893-896. doi:10.1007/s13187-019-01539-w
- Marsiglio JA, Rosenberg DM, Rooney MK, et al. Mentorship initiatives in radiation oncology: a scoping review of the literature. Int J Radiat Oncol Biol Phys. 2021;110(2):292-302. doi:10.1016/j.ijrobp.2020.12.049
- Rallis KS, Wozniak A, Hui S, et al. Mentoring medical students towards oncology: results from a pilot multi-institutional mentorship programme. J Cancer Educ. 2022;37(4):1053-1065. doi:10.1007/s13187-020-01919-7
- Kahn JM, Sandhu N, von Eyben R, et al. Radiation oncology virtual education rotation (ROVER) for medical students. Int J Radiat Oncol Biol Phys. 2021;111(1):29-35. doi:10.1016/j.ijrobp.2021.03.057
- Sandhu N, Frank J, von Eyben R, et al. Virtual radiation oncology clerkship during the COVID-19 pandemic and beyond. Int J Radiat Oncol Biol Phys. 2020;108(2):444- 451. doi:10.1016/j.ijrobp.2020.06.050
- Franco I, Oladeru OT, Saraf A, et al. Improving diversity and inclusion in the post–coronavirus disease 2019 era through a radiation oncology intensivesShadowing experience (RISE). Adv Radiat Oncol. 2020;6(1):100566. doi:10.1016/j.adro.2020.09.006
- Franco I, Oladeru OT, Saraf A, et al. RISE: an equity and inclusion-based virtual pipeline program for medical students underrepresented in medicine. Int J Radiat Oncol Biol Phys. 2021;111(1):e8. doi:10.1016/j.ijrobp.2021.05.149
- Jeans EB, Brower JV, Burmeister J, et al. Radiation oncology deliberative curriculum inquiry: feasibility of a national delphi process. Int J Radiat Oncol Biol Phys. 2021;111(1):e7. doi:10.1016/j.ijrobp.2021.05.147
- Gillespie EF, Panjwani N, Golden DW, et al. Multi-institutional randomized trial testing the utility of an interactive three-dimensional contouring atlas among radiation oncology residents. Int J Radiat Oncol Biol Phys. 2017;98(3):547-554. doi:10.1016/j.ijrobp.2016.11.050
- Eansor P, Norris ME, D’Souza LA, et al. Is remote learning as effective as in-person learning for contouring education? A prospective comparison of face-to-face versus online delivery of the anatomy and radiology contouring bootcamp. Int J Radiat Oncol Biol Phys. 2022;112(3):590-599. doi:10.1016/j.ijrobp.2021.10.011
- Winter JD, Adleman J, Purdie TG, Heaton J, McNiven A, Croke J. An innovative learning tool for radiation therapy treatment plan evaluation: implementation and evaluation. Int J Radiat Oncol Biol Phys. 2020;107(4):844-849. doi:10.1016/j.ijrobp.2020.03.018
- Li BC, Chew J, Wakefield DV, Agarwal A, Jhingran A. Frameworks for radiation oncology global health initiatives in US residency programs. JCO Global Oncology. 2021;(7):233-241. doi:10.1200/GO.20.00315
- Yeung A, Greenwalt J. A framework for quality improvement and patient safety education in radiation oncology residency programs. Pract Radiat Oncol. 2015;5(6):423-426. doi:10.1016/j.prro.2015.07.008
- Brower JV, Chen S, Ritter A, et al. Comfort level of US radiation oncology graduates: assessment of transition to independent clinical practice. J Cancer Educ. 2021;36(2):278-283. doi:10.1007/s13187-019-01625-z
- Kahn JM, DiazGranados D, Fields EC. Transitioning roles from residency to attending physician in radiation oncology. J Cancer Educ. 2022;37(4):1179-1185. doi:10.1007/s13187-020-01936-6
- Nabavizadeh N, Burt LM, Mancini BR, et al. Results of the 2013-2015 association of residents in radiation oncology survey of chief residents in the United States. Int J Radiat Oncol Biol Phys. 2016;94(2):228-234. doi:10.1016/j.ijrobp.2015.10.014
- Samuels S. First-year fears and fundamentals: an open letter to new radiation oncologists. App Radiat Oncol. 2019;8(1):31-36.
- Best LR, Sengupta A, Murphy RJL, et al. Transition to practice in radiation oncology: mind the gap. Radiother Oncol. 2019;138:126-131. doi:10.1016/j.radonc.2019.06.012
- Turner SL, Tesson S, Butow P, Vachan B, Chan MK, Shaw T. Integrating leadership development into radiation oncology training: a qualitative analysis of resident interviews. Int J Radiat Oncol Biol Phys. 2022;113(1):26-36. doi:10.1016/j.ijrobp.2021.09.051
- Akthar AS, Hellekson CD, Ganai S, et al. Interdisciplinary oncology education: a national survey of trainees and program directors in the United States. J Cancer Educ. 2018;33(3):622-626. doi:10.1007/s13187-016-1139-6
- Ni L, Thomas HR, Raleigh DR, Boreta LC, Park CC, Braunstein SE. Residents-as-teachers curriculum for radiation oncology: a targeted needs assessment. Int J Radiat Oncol Biol Phys. 2021;111(3):638-642. doi:10.1016/j.ijrobp.2021.06.024
- American Society for Radiation Oncology. ASTRO-ARRO meet me in treatment planning webinars. Published online November 19, 2019. Accessed August 29, 2022. https://www.astro.org/Affiliate/ARRO/Resident-Resources/Educational-Resources/Webinars/ASTRO-ARRO-Meet-Me-in-Treatment-Planning-Webinars
- Dean M, Jimenez R, Mellon E, Fields E, Yechieli R, Mak R. CB-CHOP: a simple acronym for evaluating a radiation treatment plan. Appl Radiat Oncol. 2017;6(4):28-30.
- Wu SY, Sath C, Schuster JM, et al. Targeted needs assessment of treatment planning education for United States radiation oncology residents. Int J Radiat Oncol Biol Phys. 2020;106(4):677-682. doi:10.1016/j.ijrobp.2019.11.023
- Padilla L, Burmeister JW, Burnett OL, et al. Interprofessional image verification workshop for physician and physics residents: a multi-institutional experience. Int J Radiat Oncol Biol Phys. 2021;111(4):1058-1065. doi:10.1016/j.ijrobp.2021.07.1706
- Leo AND, Ryckman JM, Fields EC, et al. Treatment plan evaluation workshops for residents: learning the ROPES (radiation oncology plan evaluation school). Int J Radiat Oncol Biol Phys. 2022;114(1):e8. doi:10.1016/j.ijrobp.2022.06.012
- Song EY, Chuang J, Frakes JM, et al. Developing a dedicated leadership curriculum for radiation oncology residents. J Cancer Educ. Published online February 22, 2021. doi:10.1007/s13187-021-01980-w
- Berriochoa C, Amarnath S, Berry D, Koyfman SA, Suh JH, Tendulkar RD. Physician leadership development: a pilot program for radiation oncology residents. Int J Radiat Oncol Biol Phys. 2018;102(2):254-256. doi:10.1016/j.ijrobp.2018.05.073
- Turner S, Janssen A, Chan MK, et al. Can radiation oncologists learn to be better leaders? Outcomes of a pilot foundations of leadership in radiation oncology pro- gram for trainees delivered via personal electronic devices. J Med Imaging Radiat Oncol. 2018;62(6):847-853. doi:10.1111/1754-9485.12793
- Ni L, Thomas H, Sinha S, Braunstein S, et al. Determining the feasibility and effectiveness of a virtual interactive residents-as-teachers curriculum: a proposed pilot study. Int J Radiat Oncol Biol Phys. 2022;114(1):e10. doi:10.1016/j.ijrobp.2022.06.017
- Saraf A, Sim AJ, DeLeo AN, et al. Teaching mentoring in radiation oncology (TEAMRO): a ROECSG GME multi-institutional pilot study on teaching mentorship skills to residents. Int J Radiat Oncol Biol Phys. 2022;114(1):e7-e8. doi:10.1016/j.ijrobp.2022.06.011
- Stepczynski J, Holt SR, Ellman MS, Tobin D, Doolittle BR, et al. Factors affecting resident satisfaction in continuity clinical systematic review. J Gen Intern Med. 2018;33(8):1386-1393. doi:10.1007/s11606-018-4469-8
- Gangat M, Klein GW, Cohen HW, Heptulla RA. National study of continuity clinic satisfaction in pediatric fellowship training. Adv Med Educ Pract. 2013;4:165-169. doi:10.2147/AMEP.S51069
- Witherspoon L, Jalali S, Roberts MT, et al. Resident-run urology clinics: a tool for use in competency-based medical education for teaching and assessing transition-to-practice skills. Can Urol Assoc J. 2019;13(9):E279-E284. doi:10.5489/cuaj.5710
- Lister JR, Friedman WA, Murad GJ, Dow J, Lombard GJ, et al. Evaluation of a transition to practice program for neurosurgery residents: creating a safe transition from resident to independent practitioner. J Grad Med Educ. 2010;2(3):366-372. doi:10.4300/JGME-D-10-00078.1
- Jeans EB, Beard TB, Boon AL, et al. Empowering residents into independent practice: a single-institutional endeavor aimed at developing resident autonomy through implementation of a chief resident service in radiation oncology. Int J Radiat Oncol Biol Phys. 2020;107(1):23-26. doi:10.1016/j.ijrobp.2020.01.001
- Price JG, Moravan MJ, Boyer MJ, et al. Facilitating the transition to independent radiation oncology practice through a resident-led, veterans affairs teaching hospital service. Pract Radiat Oncol. 2021;11(6):441-447. doi:10.1016/j.prro.2021.08.006
- Yoo SK, Bian SX, Lin E, et al. Development of a radiation oncology resident continuity clinic to improve clinical competency and patient compliance. Int J Radiat Oncol Biol Phys. 2018;100(3):551-555. doi:10.1016/j.ijrobp.2017.11.034
- American Board of Radiology. ABR eliminating SA-CME requirement for OLA participants. theabr.org. Published March 29, 2022. Accessed September 29, 2022. https://www.theabr.org/blogs/abr-eliminating-sa-cme-requirement-for-ola-participant
- Sherer MV, Lin D, Puri K, et al. Development and usage of eContour, a novel, three-dimensional, image-based website to facilitate access to contouring guidelines at the point of care. JCO Clin Cancer Inform. 2019;3:1-9. doi:10.1200/CCI.19.00041
- McClelland S, Chernykh M, Dengina N, et al. Bridging the gap in global advanced radiation oncology training: impact of a web-based open-access interactive three- dimensional contouring atlas on radiation oncologist practice in russia. J Cancer Educ. 2019;34(5):871-873. doi:10.1007/s13187-018-1388-7
- Franco I, Petereit DG, Mourtada F, Singer L, et al. Increasing brachytherapy mentorship and representation through #NextGenBrachy. Int J Radiat Oncol Biol Phys. 2021;111(1):e15. doi:10.1016/j.ijrobp.2021.05.163
- Brenneman RJ, Goddu SM, Andruska N, et al. Feasibility of same-day prostate fiducial markers, perirectal hydrogel spacer placement, and computed tomography and magnetic resonance imaging simulation for external beam radiation therapy for low-risk and intermediate-risk prostate cancer. Pract Radiat Oncol. 2022;12(2):e117-e122. doi:10.1016/j.prro.2021.09.015
- Green OL, Henke LE, Hugo GD, et al. Practical clinical workflows for online and offline adaptive radiation therapy. Semin Radiat Oncol. 2019;29(3):219-227. doi:10.1016/j.semradonc.2019.02.004
- Lamb J, Cao M, Kishan A, et al. Online adaptive radiation therapy: implementation of a new process of care. Cureus. 2017;9(8):e1618. doi:10.7759/cureus.1618
- Kang J, Thompson RF, Aneja S, et al. National cancer institute workshop on artificial intelligence in radiation oncology: training the next generation. Pract Radiat Oncol. 2021;11(1):74-83. doi:10.1016/j.prro.2020.06.001
- Hosny A, Bitterman DS, Guthier CV, et al. Clinical validation of deep learning algorithms for radiotherapy targeting of non-small-cell lung cancer: an observational study. Lan Dig Heal. 2022;4(9):e657-e666. doi:10.1016/S2589-7500(22)00129-7
- Wong J, Huang V, Wells D, et al. Implementation of deep learning-based auto-segmentation for radiotherapy planning structures: a workflow study at two cancer centers. Radiat Oncol. 2021;16(1):101. doi:10.1186/s13014-021-01831-4
- van der Veen J, Willems S, Deschuymer S, et al. Benefits of deep learning for delineation of organs at risk in head and neck cancer. Radiother Oncol. 2019;138:68-74. doi:10.1016/j.radonc.2019.05.010
- Ma C, Zhou J, Xu X, et al. Deep learning-based auto-segmentation of clinical target volumes for radiotherapy treatment of cervical cancer. J Appl Clin Med Phys. 2021;23(2):e13470. doi:10.1002/acm2.13470
- Duan J, Bernard M, Downes L, et al. Evaluating the clinical acceptability of deep learning contours of prostate and organs-at-risk in an automated prostate treatment planning process. Med Phys. 2022;49(4):2570-2581. doi:10.1002/mp.15525
- Li X, Zhang J, Sheng Y, et al. Automatic IMRT planning via static field fluence prediction (AIP-SFFP): a deep learning algorithm for real-time prostate treatment planning. Phys Med Biol. 2020;65(17):175014. doi:10.1088/1361-6560/aba5eb
- Li X, Wang C, Sheng Y, et al. An artificial intelligence-driven agent for real-time head-and-neck IMRT plan generation using conditional generative adversarial network (cGAN). Med Phys. 2021;48(6):2714-2723. doi:10.1002/mp.14770
- Kiser KJ, Fuller CD, Reed VK, et al. Artificial intelligence in radiation oncology treatment planning: a brief overview. J Med Artif Intel. 2019;2(0). doi:10.21037/ jmai.2019.04.02
- Carin L. On Artificial intelligence and deep learning within medical education. Acad Med. 2020;95(11S):S10. doi:10.1097/ACM.0000000000003630
- Khalid S, Goldenberg M, Grantcharov T, Taati B, Rudzicz F. Evaluation of deep learning models for identifying surgical actions and measuring performance. JAMA Netw Open. 2020;3(3):e201664. doi:10.1001/jamanetworkopen.2020.1664
- Janopaul-Naylor J, Qian D, Khan M, et al. Virtual away rotations increase access to radiation oncology. Pract Radiat Oncol. 2021;11(5):325-327. doi:10.1016/j. prro.2021.06.002
- Kahn JM, Fields EC, Pollom E, et al. Increasing medical student engagement through virtual rotations in radiation oncology. Adv Radiat Oncol. 2021;6(1):100538. doi:10.1016/j.adro.2020.07.015
- Tye KE, Williams VM, Franco I, et al. Filling a void: the creation of the ARRO equity and inclusion subcommittee. App Radiat Oncol. 2020;9(3):4.
- Kamran SC, Niemierko A, Deville C, Vapiwala N, et al. Diversity trends by sex and underrepresented in medicine status among US radiation and medical oncology faculty over 5 decades. JAMA Oncol. 2022;8(2):221-229. doi:10.1001/jamaoncol.2021.6011
- Beltrán Ponce SE, Thomas CR, Diaz DA, et al. Social determinants of health, workforce diversity, and financial toxicity: a review of disparities in cancer care. Curr Probl Cancer. Published online August 6, 2022:100893. doi:10.1016/j.currproblcancer.2022.100893
- Mattes MD, Deville C, et al. A survey to assess and delineate approaches to medical student outreach to promote diversity at academic radiation oncology programs.Int J Radiat Oncol Biol Phys. 2022;112(5):1083-1089. doi:10.1016/j.ijrobp.2021.12.165
- Powell C, Yemane L, Brooks M, et al. Outcomes from a novel graduate medical education leadership program in advancing diversity, equity, and inclusion. J Grad Med Educ. 2021;13(6):774-784. doi:10.4300/JGME-D-21-00235.1
- Damast S, Felder S, Fields E, Singer L. Feasibility of deploying a U.S. simulation-based gynecological brachytherapy educational workshop to an international setting. Brachytherapy. 2020;19(6):777-782. DOI:10.1016/j.brachy.2020.09.015. Epub 2020 Nov 19.
Citation
Saraf A, Boyd G, De Leo A, Gawu PD, Pinnix CC, Braunstein S, Jimenez R, Franco I, Singer L. Future of Radiation Oncology Education: Transforming Scholarly Teaching Into Medical Education Scholarship. Appl Radiat Oncol. 2023;(1):5-13.
March 21, 2023

Latest Review Articles
- A Narrative Review on Radiation Oncology Physician Well-Being in the United States
- A Novel Framework to Define and Prognosticate Visual Outcomes Following Fractionated Radiation Therapy for Optic Nerve Sheath
- A Practical Method to Prolong Expiratory Breath Holds for Abdominal Stereotactic Body Radiation Therapy
- Radiation Therapy-Induced Toxicity in a Breast Cancer Patient With Variance of Unknown Significance in the Ataxia Telangiectasia
- Late Effects of Pelvic Radiation Therapy in the Female Patient: A Comprehensive Review