Target tumors, not yourself: A review of False Claims Act allegations against radiation oncologists
Images
The Department of Justice is investigating radiation oncology service providers. Why? In the words of the infamous American bank robber Willie Sutton, “because that’s where the money is.” Last year, the Centers for Medicare & Medicaid Services (CMS) disclosed the amounts paid to physicians, and radiation oncologists were among the top recipients of federal monies.1 Each year, CMS pays hundreds of millions in radiation oncology claims, which steadily rise with the growing use of complex and costly radiation treatments secondary to rapidly evolving technologies. As a result, the Department of Justice and plaintiff attorneys have pursued lawsuits against radiation oncology providers with claims of fraud, abuse and waste.
This article provides an overview of the federal False Claims Act and discusses specific legal actions pursued against radiation oncology providers under the False Claims Act, either by the Department of Justice, a qui tam relator (one who brings an action on the government’s behalf), or both. Most importantly, it examines the specific misconduct identified as actionable, and highlights common sense practices to avoid being named as a False Claims Act defendant, particularly when developing cost-containment strategies.
Overview of the False Claims Act
The False Claims Act, originally known as the “Informer’s Act” or the “Lincoln Law,” was enacted in 1863 at the height of the Civil War primarily to combat fraud allegations in the United States’ procurement of Union Army supplies. The damages and penalties available under the False Claims Act are significant, and the misconduct actionable under the False Claims Act is broad and sweeping.
The False Claims Act is a federal statute that reaches not only the sub-mission of a false claim, but also the making of a record or statement to obtain payment or approval of a false claim, the possession of property or money used to defraud the government, illegal purchases from a government officer or employee, and the making of a false record to “conceal, avoid or decrease” a financial obligation to the government.2 The popularity of the False Claims Act as an anti-fraud weapon is due, in part, to the government’s ability to obtain sizeable recoveries through treble damages and penalties of up to $11,000 per claim.
The most common act prohibited by the False Claims Act is where a person presents, or causes another to present, a false or fraudulent claim for payment, and the person involved knows the claim is false or fraudulent. Knowingly means 1) having knowledge 2) acting in deliberate ignorance of the truth or falsity of the information, or (3) acting in reckless disregard of the truth or falsity of the information. No proof of specific intent to defraud is required.3 The government does not need to pay the claim for False Claims Act liability to arise. Also, penalties may be assessed even when there is no proof of damage to the United States.
In general, liability under the False Claims Act extends to deliberate ignorance and reckless disregard of the truth or falsity of information pertaining to claims for government funds. Deliberate ignorance requires proving that a provider would have had reason to believe its actions may have been unlawful and that the providers purposely failed to investigate any suspicions. In determining whether there was reckless disregard, courts have considered “clumsiness,” “carelessness and foolishness in the extreme,” “lack of slight diligence or care” and “omission in reckless disregard of a legal duty.”4
The False Claims Act has been used in a variety of contexts against government contractors, Medicare providers, real estate developers, and other providers of goods and services procured by the federal government. Several states have enacted their own versions of the federal civil False Claims Act as well.
Qui Tam provision
Under the qui tam provision of the False Claims Act, a private person may bring a civil action on behalf of the United States. The plaintiff or “relator” must provide the Department of Justice with a copy of the complaint and a written disclosure of all material evidence and information known to the relator. The complaint remains under seal for at least 60 days, during which time the Department of Justice attorneys decide to either proceed with or decline to take over the action, leaving the relator with the right to conduct the action once the complaint is unsealed. The relator is entitled to a portion of the damages recovered in the action, regardless of whether the government proceeds with it. The relator’s recovery can range from 10% to 25% of the proceeds, and may also include attorney fees.
The statute of limitations in the False Claims Act is the longer of either 6 years from the date of violation, or 3 years from the date “when facts material to the right of action are known or reasonably should have been known” by the government, but in “no event more than 10 years after the violation is committed.”5 This unique statute of limitations provision is applicable when the government fails to detect false claims at the time they are submitted because of the very deceptive nature of the fraudulent conduct.
Whistleblower protection
In the “whistleblower protection” provision, the False Claims Act creates a federal cause of action for any employee retaliated against by an employer for aiding in a False Claims Act prosecution.6 Importantly, this cause of action is not limited to qui tam relators. As a result of an amendment to the original law, it covers any employee, contractor, agent or associated others. The amendment allows an action for retaliation to be based on relationships outside the traditional employer-employee relationship. Any protected individual who investigates, initiates, testifies, or assists in a False Claims Act action can bring a cause of action.7
A person who proves the necessary elements of a retaliation claim is entitled to “all legal relief necessary to make the employee whole,” including “reinstatement with the same seniority status … 2 times the amount of back pay, interest on back pay, and compensation for any special damages.”7 The statute of limitations for a retaliation action is 3 years after the date the retaliation occurred. Several examples below involve claims following the termination of an employee who identified the alleged misconduct.
Department of Justice’s role in a qui tam complaint
Once the government receives a qui tam complaint along with material evidence and information, it has several options. First, it can request an extension of the 60-day sealing period. Second, it can elect to intervene and take over the action. Third, it can notify the court that it declines to intervene, permitting the relator to conduct the action in place of the government. Fourth, it can move to dismiss or stay the qui tam relators proceeding with the matter on the grounds that action would interfere with an ongoing criminal investigation. Finally, the government can attempt to settle the action before declaring its formal intervention decision. Even if the government initially declines to intervene, it can do so later upon showing good cause.8
If the government elects to intervene in a False Claims Act qui tam proceeding, the government files its complaint in intervention, which generally includes the allegations identified in the original qui tam complaint. The government’s complaint may add or delete certain allegations and parties, and plead specific common law claims, such as common law fraud, breach of contract, and unjust enrichment, which a relator cannot bring in a qui tam proceeding for lack of standing, an enforceable legal right to such claims.
When the government intervenes, the question may arise as to whether those newly pleaded claims relate back to the filing of the original qui tam complaint or may be barred by the statute of limitations. The False Claims Act provides that the government’s complaint relates back to the date of the qui tam relator’s complaint “to the extent that the claim of the Government arises out of the conduct, transactions, or occurrences set forth … in the prior complaint.”9
Settlement of False Claims Act cases
What makes a False Claims Act proceeding most unique is that the subject of a False Claims Act investigation may have to simultaneously defend against a criminal investigation, a civil False Claims Act action, and the administrative threat of suspension or the outright exclusion from government programs. Accordingly, the subject of a False Claims Act inquiry must view the implications of a False Claims Act investigation as a serious matter.
Because False Claims Act investigations may involve civil, administrative, criminal and a variety of state common law allegations (including claims raised under any applicable state false claims act laws), the resolution of parallel criminal and administrative claims is often sought in approaching a global settlement. The resolution of parallel criminal and administrative claims is also critical to avoiding potential suspension or debarment, or outright exclusion from federal programs. As a result, a False Claims Act defendant will often try to resolve all outstanding civil, criminal and administrative claims relating to the alleged false claims when settling a civil False Claims Act matter.
The Department of Justice, in contrast, typically offers only a narrow release out of concern that a broader release may capture claims not fully investigated. Further, the Department of Justice declines to release False Claims Act defendants from potential suspension and debarment proceedings when settling civil False Claims Act cases. In the healthcare arena, issues relating to exclusion from federal healthcare programs must be negotiated within the exclusive authority of the Department of Health and Human Services. This often requires separate, independent negotiations with the excluding or debarring authority who will need to evaluate the case and determine whether to settle permissive exclusion issues arising from the False Claims Act settlement once reached. Often, the excluding agency will require that the False Claims Act defendant demonstrate that it has internal compliance procedures sufficient to protect against future misconduct. If not, the False Claims Act defendant may be required to adopt a corporate integrity agreement, which may require an independent monitor to ensure that future misconduct will not occur. Such corporate integrity agreements can be onerous and expensive for a provider.
Recently settled qui tam actions involving radiation oncology providers
The claim for medically unnecessary services — those not properly supervised, or lacking proper documentation supporting the service — is typically the basis for recent False Claims Act actions against radiation oncology providers. Medicare reimburses, and participating providers agree to submit, claims only for services medically necessary to diagnose and treat an illness or injury, and for which the provider maintains adequate documentation justifying treatment.10 Services performed without appropriate supervision are not considered reasonable and necessary and, therefore, are not covered under Medicare.11 Failure to provide required supervisory care renders the service nonreimbursable because the services are deemed medically unnecessary.12 The 3 levels of supervision (general, direct and personal) should be well known to all radiation oncology practitioners as they relate to services.13
A False Claims Act requires specific allegations concerning the allegedly fraudulent behavior of the defendants. Recently filed actions against radiation oncology providers all contain a common allegation: lack of, or improper supervision of procedures requiring either direct supervision (e.g., daily treatments, simulations and intensity-modulated radiation therapy [IMRT]) or personal supervision (e.g., stereotactic body radiation therapy [SBRT], radiosurgery, or brachytherapy). In addition to submitting claims for services provided when the physician was not present, some actions demonstrate the incredulous lengths to which providers have taken to circumvent supervision requirements. Other False Claim Actions allegations include overuse of CPT codes, illegal kickbacks, improper referrals, failure to provide appropriate services, improper treatment, and lack of operable equipment.
Some of the complaints below are relatively straightforward with simple fact patterns, while others are much more involved. We must stress that the cases and claims were allegations only, as contained in the complaints filed in district courts, and have been settled with no determination of liability.
United States ex rel. Refaei v. Vantage Oncology and Associates, Inc., United States District Court S.D. of Ohio, Case No: 1:10-cv-833
This case offers comprehensive allegations and alleged multiple schemes which, for simplicity, are summarized as follows:
Failure to render required supervisory care. Claims for treatment were submitted during periods when the physician was on vacation and or was at centers other than those where patients were treated and billed. In one instance, a patient undergoing treatment died with no physician available to aid in resuscitation efforts. To create the illusion of physician presence during treatment, “GoToMyPC” software was used despite a compliance officer’s recognition that “virtual” review did not satisfy image-guided radiation therapy (IGRT) or IMRT supervision requirements. (Prior to 2009 — the time period for a majority of the claims in the Refaei complaint — IGRT required personal supervision, and subsequent to January 1, 2009, IGRT required direct physician supervision; IMRT required and continues to require direct supervision.)
Submitting false claims for services inappropriately administered and/or improperly documented treatment. Postimplant prostate brachytherapy dosimetry revealed multiple patients receiving > 20% of the prescribed dose (1 patient received > 170% of prescribed dose) which, upon discovery, should have triggered medical event reporting. The relator reported the events to a vice president of medical physics and noted that the events were covered up by creating a second patient chart so the medical events were not reflected in records or reports. The relator claimed he was reprimanded after e-mailing the physician, requesting an independent peer review of the brachytherapy cases.
Overuse/overbilling. Allegations of routinely billing special treatment procedure (77470) charges for many patients without any documentation and policy of billing special medical radiation physics consult (77370) for most IMRT plans without a documented physician request or signature. The complaint alleged that a graduate physicist performed the physics consults but had the vice president of physics (who was not personally involved and out of state) sign plans; alleged pressure to bill special dosimetry charges (77331) for each plan, averaging 3 charges for each patient, without specifying devices to be used (thermoluminescent dosimeters, diodes); and stated that many measurements were taken unnecessarily, without justification or by unqualified personnel and signed off by a physicist weekly.
Failure to document and other sundry allegations. In addition to the documentation issues above, the complaint alleged that claims were submitted for complex simulations without documentation of immobilization devices or other items that would justify the charge. Documentation was also lacking to demonstrate the training of physicists, dosimetrists and therapists, or to support the use of IMRT. Other allegations included the overutilization of IMRT (despite Vantage’s compliance department identifying inappropriate and overutilization of IMRT), lack of an operational simulator (yet charges for simulation), presence of a treating therapist who was only conditionally accredited to treat at one location, yet treated patients at another facility, and the hiring as manager someone with little or no training because he was the son-in-law of the CEO of a hospital in the planning stages of opening a radiation facility with Vantage.
Failure to perform services. Allegations that claims for other services were submitted but allegedly not performed: IMRT boost calculations, and phantom quality assurance for IMRT and computed tomography (CT) simulations (no films were obtained as the simulator was nonfunctional).
United States ex rel. Berger et al v Baylor University Medical Center at Dallas et al., United States District Court N.D. Texas, Case No: 3:10-cv-1103
This case involved a qui tam action brought by a radiation oncologist and radiation therapist alleging violation of physician supervision requirements at Baylor’s radiosurgery center as well as violation of the Anti-kickback Statute and Stark Act.
Documentation supported Baylor and Texas Oncology’s knowledge of supervision requirements for radiosurgery procedures, yet Baylor relaxed its existing supervision rules to allow Texas Oncology (TO) physicians to see patients at another location contemporaneous with ongoing radiosurgery procedures at the Baylor Radiosurgery Center. Physicians’ patient schedules from both locations were available, documenting where physicians were (and were not) during radiosurgery cases.
The relators raised safety and supervisory concerns with top management of Baylor, Health Texas and TO, alleging that supervision concerns were overridden by financial incentives. In support of this claim, available meeting minutes of Baylor’s radiosurgery council implicitly admitted knowledge of the supervision rules, granting permission for necessary physicians to be available by phone as a supervision rule workaround. At times, only a nurse and medical physicist were present during radiosurgery procedures, including a situation when a Gamma Knife (Elekta, Stockholm, Sweden) patient’s condition changed, warranting transfer to the emergency room.
In another supervision workaround, Baylor misrepresented the training and education of the neurosurgeons and an otolaryngologist when including them on its radioactive material license to act as qualified users during Gamma Knife procedures, thereby accommodating TO radiation oncologists to see patients elsewhere.
Not only did the relator, concerned about patient safety, make management aware of the supervision and qualification rules, he also reported his discussions with the University of Pittsburgh Medical Center (UPMC), a center that remedied its supervision procedures after being cited by the Nuclear Regulatory Commission (NRC) for not meeting requirements. For his actions, the relator’s contract was not renewed.
Overlooking supervision rules was alleged to be an inducement to refer radiosurgery and chemotherapy patients to Baylor, constituting illegal kickbacks under the Anti-Kickback Statute and violating the Stark Act. Also alleged as an inducement was the naming of a TO radiation oncologist as an associate director of Baylor’s radiosurgery center even though he would not have any management or supervisory role — a position allegedly created as a means of inducing referrals for financial gain (Baylor owned the equipment so it received the technical fees).
Lastly, unbundling CyberKnife (Accuray, Sunnyvale, California) treatment codes was alleged, creating “fake” treatment plans (prior to 2006, billing planning codes separately from global codes on the treatment’s date was banned) and failure to perform daily quality assurance and/or backdating test results.
United States ex rel. Koch v. Gulf Region Radiation Oncology Centers Inc. (GRROC) et al., United States District Court N.D. Fla. Case No. 3:12-cv-0050
This case involved a $3.5 million settlement and supervision claims. For nearly 4 years, 2 radiation oncologists (GRROC) provided services for 3 locations; when on vacation, only 1 physician was available for the 3 locations. Of the 3 centers, one (Sacred Heart) contracted with GRROC to provide radiation services. When issues of coverage and billing were brought to the attention of Sacred Heart management, neither Sacred Heart nor GRROC were willing to pay for additional coverage or change billing practices. Not only were supervision claims brought for simulations, treatments and other procedures, but also, similar to other qui tam actions, the usual litany of claims related to lack of medical necessity documentation and/or routine claims on all patients for special physics consults, treatment procedures, devices and unbundling of IMRT-related charges were raised. Also similar to Refaei, allegations that no physician was present when a patient required transport to the emergency room strengthened the relator’s allegations against GRROC.
United States ex rel. Montejo v. Adventist Health System et al., United States District Court M.D. Fla. Case No. 8:13-cv-00206
Inappropriate supervision as well as lack of supervision claims were among those alleged in this case, which settled for $5.4 million this year. The relator was a radiation oncologist who brought suit against his employer, Florida Oncology Network (FON), and the hospital system for which FON provided radiation oncology professional services. The complaint alleged that FON lacked sufficient radiation oncologists to be present at each of its multiple facilities, instead relying on nearby emergency room physicians, unaffiliated medical oncologists, nurse practitioners and physician assistants. Anywhere from 10 to 15 patients per day up to 80 to 100 patients per day were treated at sites covered by FON. None of the sites were scheduled to have full-time coverage by radiation oncologists except the location with the fewest patients on treatment; this was the only site where FON collected all technical and professional revenue. Two sites were scheduled to be covered by only 1 radiation oncologist simultaneously, and other physicians were scheduled to perform brachytherapy/IORT (intra-operative radiation therapy) simultaneously while external-beam patients were undergoing treatment.
As in the other actions, a patient sustained an injury at a site without a nurse or radiation oncologist present, at which time the presumed supervising, unaffiliated medical oncologist refused to offer medical attention. A more serious allegation concerned the simulation of a spine, where evidence of prior radiation could have been noted had a radiation oncologist been present, resulting in a patient’s paraplegia secondary to radiation necrosis of the spinal cord due to re-irradiation. Similar to other actions presented here, the complaint reiterated investigations of radiation mishaps as reported in numerous newspaper articles.
The relator’s concerns of appropriate coverage and patient safety made known to management were met with the response that patient volumes did not justify the cost of additional physician coverage. In addition, a biller’s notice to management regarding supervision requirements were acknowledged, but ignored. When CMS inspectors were on site and for on-treatment visits (OTVs)days, Adventist published a radiation oncology coverage schedule, using initials only, to create the illusion that there was full coverage at all times. Some of the initials referred to physician assistants and nurse practitioners, not radiation oncologists.
Similar to other actions referenced, allegations regarding the routine use/billing for IGRT on palliative cases (such as whole brain) and IMRT for breast boosts were made. Unique to this action was the allegation that weekly management charges were billed when a nurse or physician assistant, and not the physician, saw the patient on OTV.
United States ex rel. Ana v. Winter Park Urology, et al., United States District Court M.D. Fla. Case No. 6:10-cv-00806
Not all actions resulted in settlements against all named defendants. The radiation oncologists who contracted with Winter Park Urology were successful in having the complaint against them dismissed on the eve of trial. This action alleged inappropriate physician supervision, unlike the preceding actions alleging inappropriate supervision by nonphysicians or absence of any physician during treatment.
Winter Park Urology contracted with a group of radiation oncologists (ROC) to perform radiation oncology services at its Orlando Cancer Institute (often referred to as a “urorad center”). The radiation therapists and administrators were employees of Winter Park Urology, which owned the radiation equipment. ROC operated its own radiation facility in Sanford, unrelated to the Orlando Cancer Institute. About 15% to 20% of the patients treated at the Orlando Cancer Institute had nonurologic primaries, many of which were breast cancer.
The relator was the director of medical physics who brought to management’s attention that Orlando Cancer Institute was routinely billing for special physics consults, without having a request from the physician, as was his practice at the nonaffiliated center owned by ROC. He was fired 4 days later despite “excellent” or “outstanding” evaluations, and later brought the qui tam action alleging inappropriate billing of special physics and special treatment procedure charges routinely on all cases. In addition, he also alleged claims for inappropriate supervision.
What differentiates this supervision claim from supervision claims in other cases was that the required physician supervision was allegedly inappropriate. While a urologist was present when patients were undergoing daily radiation treatment, the radiation oncologists were not routinely on site, estimating that 35% of all radiation procedures were performed when no radiation oncologist was present. The relator alleged that a radiation oncologist was never present for IGRT (IGRT required personal supervision prior to 2009, and direct supervision beginning in January, 2009); instead, the radiation oncologist would review the images weekly. In support of his allegations, the relator produced Orlando Cancer Institute’s web page, informing patients that its radiation oncologists would perform physical and medical record examination and, if appropriate for radiation, would see patients regularly during their treatment.
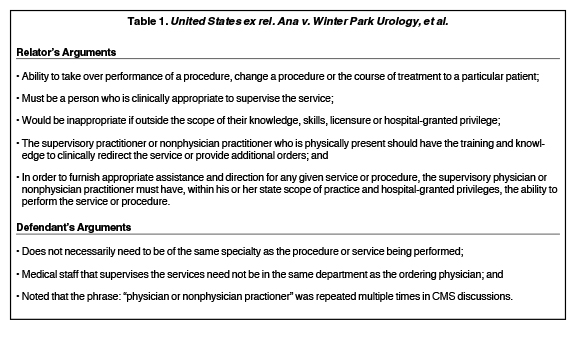
Among several theories of defense pertinent to this review, counsel for ROC argued that there was ambiguity as to the physician supervision requirements. Counsel asserted there was no CMS requirement that a radiation oncologist, and only a radiation oncologist, was required to provide supervision of the daily radiation treatments. In addition to relying on CMS discussions, counsel also argued that the term “clinically appropriate” was ambiguous and not addressed by CMS. Citing case law, the relator argued that the absence of regulatory guidance was significant to showing that Winter Park Urology knowingly violated the law when interpreting that any physician (and not specifically a radiation oncologist) could supervise the services. Winter Park Urology stated that “perhaps it is better practice for a radiation oncologist to supervise IMRT or IGRT procedures; however, technical compliance with the law does not mandate this.” Lastly, the defendants argued that reckless disregard could not be established because they made reasonable inquiry, obtaining legal advice, into the meaning of the law.14
Both the relator’s complaint and defense counsel emphasized and reiterated CMS language throughout their respective pleadings, the highlights of which are summarized in Table 1. Readers are encouraged to read both 74 Fed. Reg. 60316, 60584 and 75 Fed Reg 72012. Multiple sources of legal analysis regarding these regulations exist.
Whether or not the urologists in this case had “the training and knowledge to clinically redirect the service or provide additional orders” to satisfy “direct supervision” was never adjudicated. The relator agreed to dismiss the claims against the radiation oncologists. Readers will draw their own conclusions, but should not infer any sort of legal guidance. Unfortunately, those looking for resolution regarding controversies involving urorad centers,13 including appropriate supervision, will remain in suspense.
Discussion
The most direct allegation against a radiation oncology provider is the allegation of lack of appropriate supervision where the claim for reimbursement requires a level of supervision not provided. Brachytherapy, radiosurgery and SBRT are the most frequently performed procedures requiring personal supervision. Most other radiation oncology procedures (e.g., daily treatment, IGRT and simulation) require direct supervision. No expert testimony is needed, nor is it a matter of opinion, to substantiate an allegation of lack of supervision, when the physician is on vacation or at another facility. Competing theories of expert testimony can be avoided altogether in such situations. Furthermore, when performing services requiring personal supervision, a physician is not considered “available” as required for direct supervision for any other contemporaneous treatments and/or procedures. Lack of supervision, as it relates to a physician’s presence, can be easily established through a variety of electronic and documentary evidence such as: schedules, flight itineraries, credit card statements, interviews with other staff, and cell phone records.
While the definition of personal supervision is clear (attendance in the room during the procedure) Medicare has declined to define “immediate” for purposes of direct supervision in terms of time or distance. Defining “immediate” is beyond the scope of this article and the reader is directed to appropriate legal commentary.15,16 Reports of radiation mishaps that occur secondary to a physician’s lack of supervision are reported in the general media.17 The tragic results reported in the referenced article were reiterated in the body of one of the qui tam actions discussed here,18 emphasizing that the lack of a physician’s presence during treatment is an effectively damaging and easily proven allegation.
Appropriate supervision is another matter, given the contentious discussion in the general media 19,20 and within professional medical societies involving “urorad centers,” as this may not be well settled as in the qui tam action presented above.21 It is clear that physicians lacking specified training may not be listed on a radioactive materials license (e.g., otolaryngologists, as in Baylor). While it may be a reach to suggest that ER physicians, nurses and assistants possess adequate therapeutic radiation training, the question of who may be appropriately qualified or privileged has not been conclusively answered in regulations or law.
CMS requires hospitals to carefully consider who are appropriate candi-dates (physicians and other healthcare practitioners) when appointing medical staff to practice at the hospital in accordance with state law. CMS requires that hospital committees examine credentials of all candidates, and make recommendations for medical staff membership and privileges to the hospital’s governing body as a part of its Conditions of Participation and Conditions for Coverage that health care organizations must meet to begin and continue participating in the Medicare and Medicaid programs. The underlying premise is that health and safety standards are the foundation for improving quality and protecting the health and safety of beneficiaries.15
Another common False Claims Act allegation easily substantiated relates to claims for reimbursement that are not supported by appropriate documentation. Examples include billing for: 1) complex simulations lacking documentation of treatment/immobilization devices; 2) first-day simulations lacking documentation of physician review before treatment; and 3) special treatment procedures lacking substantiation (e.g., retreatment of a previously irradiated site, presence of medical devices in/near field, etc.). Although useful in facilitating the billing process, documentation does not always need to be written. For example, blocks, immobilization devices or the presence of devices in a treatment field can be easily identified in films or treatment plans and are, therefore, documented in the record to substantiate claims.
False Claims Act allegations that relate to kickback schemes, claims for inappropriate treatment and/or unnecessary charges present a greater evidentiary challenge to the government or qui tam relator than allegations relating to supervision or documentation. These allegations may likely require opinion testimony, which requires an expert witness. Similar to medical malpractice actions, proof required may resort to dueling experts. Such allegations may include the inappropriate use of IMRT, SBRT, Gamma Knife, physics consults and special treatment procedures. Substantiating the allegation may be easier if a particular modality was used for nearly every case, or where corporate “unwritten rules” dictate that a certain percentage of all cases must, for example, use IMRT. In addition to expert testimony, parties in an action may present National Comprehensive Cancer Network (NCCN) guidelines and care paths as another form of (pseudo) expert opinion that the trier of fact (i.e., the judge or jury) may consider in determining if services are unnecessary or inappropriate.
The easiest allegations to support, although not always financially rewarding, are those where outrageous misconduct occurs that shocks the conscience of the trier of fact. Examples presented above include: the death of a patient where no physician was present to administer aid; the failure to report untoward clinical outcomes or misadministrations; rationalizing that a virtual web or telephone presence constitutes personal supervision; the existence of alternate or “ghost” records; billing for films despite having a nonfunctional x-ray unit; record alteration; retaliation against personnel raising concerns of patient safety; hiring unqualified but connected personnel; and billing identical special charges for every patient. Allegations such as these add a certain “sex appeal” to the proceeding, which present unique challenges to the False Claims Act defendant.
Lastly, some of the allegations listed, while describing less than appropriate behavior, may not be sufficient on their own to bring an action. Examples include family connections to drive business, training levels of therapists or physicists, and frequency of any quality assurance. Some of the allegations, like overdosing or treating the wrong site (i.e., misadministration), may be covered under different civil statutes, while other allegations, like creating false charts for submission (i.e., tampering with records) may be covered by criminal statutes. Whether these allegations support a False Claims Act is not as important as how they serve to add additional color to the proceeding.
Conclusion
In improving the quality of radiation oncology practice, distilling the common mistakes alleged in False Claims Act actions reinforces what constitutes good practice, particularly with the increasing use of SBRT, which requires personal supervision by the physician along with concomitant physics and documentation requirements. A common thread woven throughout the False Claims Act cases is that each involved a qui tam relator whose quality concerns were rebuffed or outright ignored. Investigating concerns brought by relators often leads to the discovery of additional, actionable violations, which may be more easily substantiated and far more costly. This is not much different than the egregious acts allegedly committed by Al Capone that would have been much more difficult to prosecute than simple income tax evasion, which ultimately put him behind bars.
As supervision-related claims were the simplest claims to support in the above cases, supervision requirements must be adhered to, and are reasonably clear. The Office of the Inspector General and Department of Justice consider supervision important and critical to patient safety.15 Less clear is who may supervise, which is an evolving issue that may be resolved by hospitals in complying with CMS rules for Conditions of Participation with respect to privileging.22 While certain medical practices have expanded definitions of who can be privileged to perform certain procedures, cost-containment strategies that would allow anyone other than a physician trained in radiation oncology to supervise radiation treatments should be reviewed with legal counsel. CMS language, requiring “the training and knowledge to clinically redirect the service or provide additional orders,” provides prudent guidance when establishing policies.
Finally, when making decisions on how to establish clinical practices, the best guidance to follow is simple: how would this decision be perceived if alleged in a lawsuit?
References
- Weaver C, McGinty T, Radnofsky L. Small slice of doctors account for big chunk of Medicare costs. The Wall Street Journal. April 9, 2014.
- 31 U.S.C. § 3730 et seq.
- 31 U.S.C. § 3279-33.
- Doan R. The False Claims Act and the Eroding Scienter in Healthcare Fraud Litigation. Annals of Health Law. Winter 2011;1-27.
- 31 U.S.C. § 3731(b).
- 31 U.S.C. § 3730(c)(1).
- 31 U.S.C. § 3730(h).
- 31 U.S.C. § 3730(c)(3).
- 31 U.S.C. § 3731(c).
- United States ex rel. Ana v. Winter Park Urology, et al., 6:10-cv-00806. (MD Fla 2013).
- 42 U.S.C §1395y(a)(1)(A).
- 42 C.F.R. § 410.32 (b) & (d)(2).
- 42 C.F.R. § 411.15 (k)(1).
- 42 C.F.R. § 410.32(b)(3).
- Grubman SR. False Claims Act physician supervision cases on the rise. The Health Lawyer. 2014; 26(5):20-23.
- Fraud and Abuse Review 2013. Bass Berry & Sims. http://www.bassberry.com/~/media/Files/Publications/2014/02/Healthcare%20Fraud%20and%20Abuse%202013%20Year%20End%20Review.pdf. Accessed May 17, 2015.
- Bogdanich W. The radiation boom: radiation offers new cures, and ways to do harm, The New York Times. January 24, 2010.
- United States ex rel. Berger et al. v Baylor University Medical Center at Dallas et al., United States District Court N.D. Texas, Case No: 3:10-cv-1103.
- Carreyrou J, Tamman MA. Device to kill cancer, lift revenue. The Wall Street Journal. December 7, 2010.
- The New Men’s Club: Urology Radiation Centers. WSJ Video. December 7, 2010. http://www.wsj.com/video/the-new-men-club-urology- radiation-centers/428E1E4F-82ED-497D-A483-B381CFE6925E.html. Accessed May 17, 2015.
- United States ex rel. Ana v. Winter Park Urology, et al., United States District Court M.D. Fla. Case No. 6:10-cv-00806.
- 42 C.F.R. Parts 482 and 485 [CMS-3244-F] Fed Reg. Vol. 77: 95.